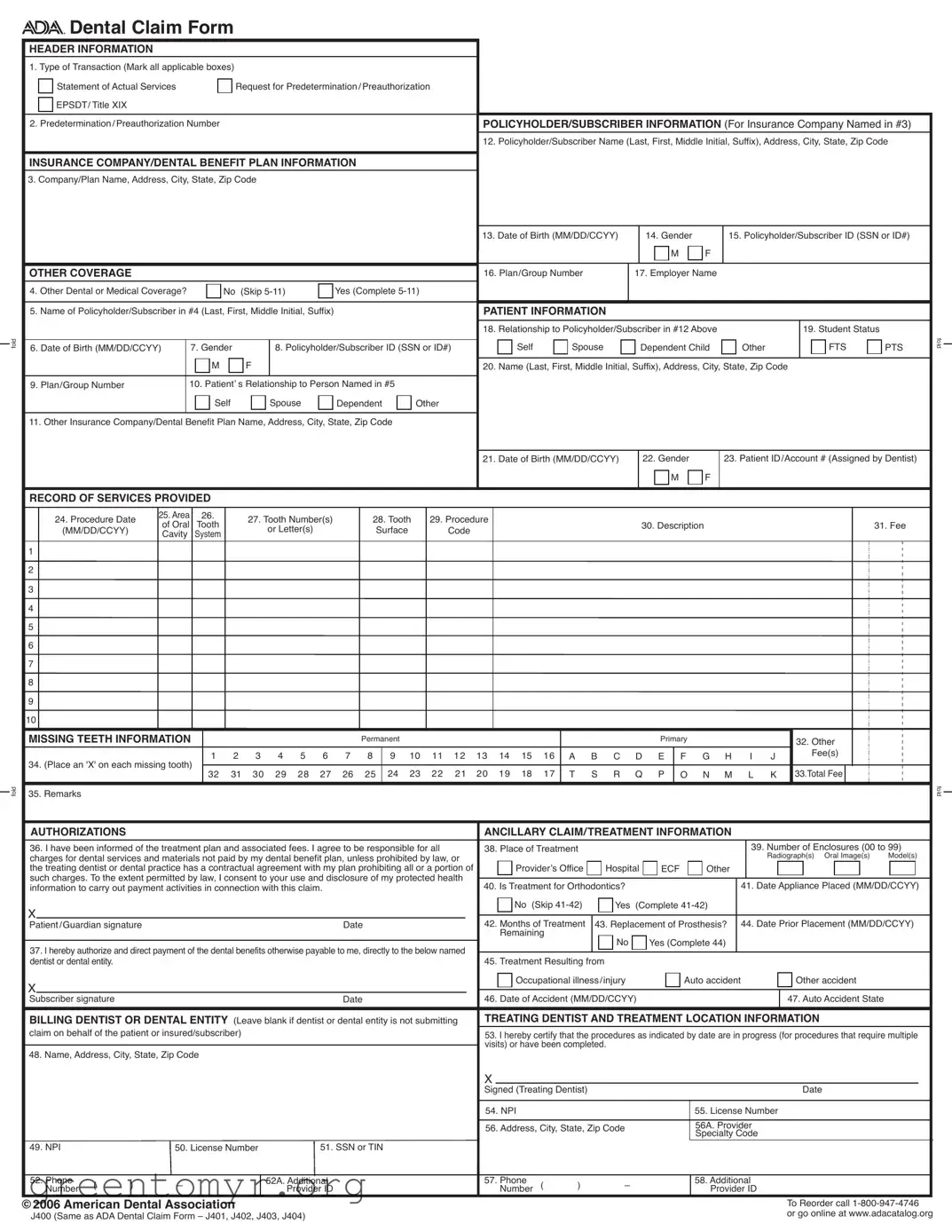
The ADA Dental Claim Form serves as a crucial document for both dental professionals and patients, streamlining the process of submitting claims to insurance companies. This form encompasses essential sections, including header information, policyholder details, patient specifics, and a record of services provided. It allows dental practices to indicate the type of transaction, such as a statement of actual services or a request for preauthorization. Policyholder information, including names, addresses, and insurance details, must be accurately filled out to ensure proper processing. Additionally, the form requires patient demographics and their relationship to the policyholder, alongside any other insurance coverage details. A comprehensive record of services, including procedure dates, descriptions, and associated fees, is vital for claims approval. The form also includes authorizations for treatment and payment, ensuring that patients understand their financial responsibilities. By adhering to the guidelines set forth in the form, dental practices can facilitate efficient claims processing, ultimately benefiting both the provider and the patient.
fold
fold
Dental Claim Form
HEADER INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
1. Type of Transaction (Mark all applicable boxes) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Statement of Actual Services |
|
|
Request for Predetermination/Preauthorization |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
EPSDT/ Title XIX |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Predetermination/Preauthorization Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
POLICYHOLDER/SUBSCRIBER INFORMATION (For Insurance Company Named in #3) |
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. Policyholder/Subscriber Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code |
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
INSURANCE COMPANY/DENTAL BENEFIT PLAN INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
3. Company/Plan Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. Date of Birth (MM/DD/CCYY) |
|
|
14. Gender |
|
|
15. Policyholder/Subscriber ID (SSN or ID#) |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
OTHER COVERAGE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16. Plan/Group Number |
|
|
17. Employer Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
4. Other Dental or Medical Coverage? |
|
|
No (Skip |
|
|
Yes (Complete |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
5. Name of Policyholder/Subscriber in #4 (Last, First, Middle Initial, Suffix) |
|
|
|
|
|
|
|
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. Relationship to Policyholder/Subscriber in #12 Above |
|
|
|
|
|
|
|
19. Student Status |
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Self |
|
Spouse |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FTS |
PTS |
fold |
|||||||||
6. Date of Birth (MM/DD/CCYY) |
|
7. Gender |
|
|
|
8. Policyholder/Subscriber ID (SSN or ID#) |
|
|
|
Dependent Child |
Other |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
M |
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
9. Plan/Group Number |
|
|
10. Patient’ s Relationship to Person Named in #5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
Self |
|
|
|
Spouse |
|
Dependent |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
11. Other Insurance Company/Dental Benefit Plan Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. Date of Birth (MM/DD/CCYY) |
|
|
22. Gender |
|
|
23. Patient ID/Account # (Assigned by Dentist) |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
RECORD OF SERVICES PROVIDED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24. Procedure Date |
25. Area |
26. |
|
27. Tooth Number(s) |
|
|
28. Tooth |
29. Procedure |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
of Oral |
Tooth |
|
|
|
|
|
|
|
|
|
30. Description |
|
|
|
|
|
|
|
|
|
|
|
31. Fee |
|
||||||||||||||||||||||||||||
|
(MM/DD/CCYY) |
|
|
|
|
or Letter(s) |
|
|
|
Surface |
Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
Cavity |
System |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
MISSING TEETH INFORMATION |
|
|
|
|
|
|
|
|
|
|
Permanent |
|
|
|
|
|
|
|
|
|
|
Primary |
|
|
|
|
|
|
|
|
|
32. Other |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
8 |
|
9 10 11 12 13 14 15 16 |
A B C D E |
F G H |
|
I |
J |
|
|
|
|
Fee(s) |
|
|
|
|
|
|
|
|||||||||||||||||||
34. (Place an 'X' on each missing tooth) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
32 |
31 |
30 |
29 |
28 |
27 |
26 |
|
25 |
|
24 23 |
22 21 |
|
20 19 18 |
17 |
T |
S R |
Q |
P |
O |
N M |
|
L |
K 33.Total Fee |
|
|
|
|
|
|
|
||||||||||||||||
35. Remarks |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
fold |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
AUTHORIZATIONS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ANCILLARY CLAIM/TREATMENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
36. I have been informed of the treatment plan and associated fees. I agree to be responsible for all |
38. Place of Treatment |
|
|
|
|
|
|
|
|
|
|
|
|
39. Number of Enclosures (00 to 99) |
|
||||||||||||||||||||||||||||||||||||||
charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Radiograph(s) Oral Image(s) |
Model(s) |
|
|||||||||||||||||||||||||||||||||
the treating dentist or dental practice has a contractual agreement with my plan prohibiting all or a portion of |
|
Provider’s Office |
Hospital |
ECF |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
such charges. To the extent permitted by law, I consent to your use and disclosure of my protected health |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
information to carry out payment activities in connection with this claim. |
|
|
|
|
|
|
|
40. Is Treatment for Orthodontics? |
|
|
|
|
|
|
|
|
|
41. Date Appliance Placed (MM/DD/CCYY) |
|
||||||||||||||||||||||||||||||||||
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No (Skip |
Yes |
(Complete |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient/Guardian signature |
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
42. Months of Treatment |
43. Replacement of Prosthesis? |
|
44. Date Prior Placement (MM/DD/CCYY) |
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Remaining |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
37. I hereby authorize and direct payment of the dental benefits otherwise payable to me, directly to the below named |
|
|
|
|
No |
|
|
Yes (Complete 44) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
dentist or dental entity. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
45. Treatment Resulting from |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Occupational illness/injury |
|
|
|
Auto accident |
|
|
|
|
|
Other accident |
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Subscriber signature |
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
46. Date of Accident (MM/DD/CCYY) |
|
|
|
|
|
|
|
|
|
|
47. Auto Accident State |
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
BILLING DENTIST OR DENTAL ENTITY (Leave blank if dentist or dental entity is not submitting |
TREATING DENTIST AND TREATMENT LOCATION INFORMATION |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
claim on behalf of the patient or insured/subscriber) |
|
|
|
|
|
|
|
|
|
|
|
|
|
53. I hereby certify that the procedures as indicated by date are in progress (for procedures that require multiple |
|
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
visits) or have been completed. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
48. Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signed (Treating Dentist) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
54. NPI |
|
|
|
|
|
|
|
|
|
55. License Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
56. Address, City, State, Zip Code |
|
|
|
|
|
56A. Provider |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Specialty Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
49. NPI |
|
|
50. License Number |
|
|
|
51. SSN or TIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
52. Phone |
( |
) |
– |
|
|
|
|
|
52A. Additional |
|
|
|
|
|
|
|
57. Phone |
( |
) |
– |
|
|
|
|
|
58. Additional |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Number |
|
|
|
|
|
|
|
Provider ID |
|
|
|
|
|
|
|
|
Number |
|
|
|
|
|
Provider ID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
©2006 American Dental Association |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To Reorder call |
|
||||||||||||||||||||
J400 (Same as ADA Dental Claim Form – J401, J402, J403, J404) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
or go online at www.adacatalog.org |
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
| Fact Name | Details |
|---|---|
| Form Purpose | The ADA Dental Claim Form is used to submit dental claims to insurance companies for reimbursement of dental services provided. |
| Transaction Types | Users can mark multiple transaction types, including Statement of Actual Services, Request for Predetermination/Preauthorization, and EPSDT/Title XIX. |
| Policyholder Information | It requires the policyholder's name, address, and identification details, ensuring that the claim is linked to the correct insurance policy. |
| Patient Relationship | The form asks for the patient's relationship to the policyholder, which can include options like self, spouse, or dependent. |
| Missing Teeth Information | Claimants must indicate missing teeth by marking an 'X' on the appropriate teeth in the designated section. |
| Authorization Requirement | Patients or guardians must sign the form, indicating they understand the treatment plan and agree to be responsible for any unpaid charges. |
| Coordination of Benefits | When applicable, the form must be completed in its entirety and the primary payer's Explanation of Benefits (EOB) attached for secondary claims. |
| National Provider Identifier (NPI) | The NPI is a unique identifier assigned to healthcare providers, including dentists, and is required for claims submission. |
| Provider Specialty Codes | Providers must enter a specialty code that indicates the type of dental professional who delivered the treatment, ensuring accurate processing. |
| State-Specific Forms | Some states may have specific requirements or variations of the ADA Dental Claim Form, governed by state laws regarding dental insurance claims. |
Completing the ADA Dental Claim form requires careful attention to detail. Follow these steps to ensure all necessary information is accurately provided.
Once you have filled out the form, review it for accuracy. Ensure that all required fields are completed and that the information matches what your dental provider has given you. After verifying everything, submit the form to the appropriate insurance company or dental benefit plan for processing.
The ADA Dental Claim Form is a standardized document used by dental providers to submit claims for payment to dental benefit plans. It captures essential information about the patient, the dental services provided, and the insurance coverage involved.
The form should be completed by the dental provider rendering the services or, in some cases, by the patient or policyholder. It requires information about the patient, the dental services performed, and the insurance details.
The header section requires the type of transaction (e.g., statement of actual services, request for predetermination), the predetermination number, and the policyholder/subscriber information, including their name, address, and insurance details.
If the patient has additional dental or medical coverage, the "Other Coverage" section must be completed. This includes the name of the policyholder and relevant details about the other insurance plan.
This section requires detailed information about the dental procedures performed, including:
Ensure that all fields are filled out accurately to avoid delays in processing the claim.
If the number of procedures exceeds the lines available on the claim form, you should list the additional procedures on a separate, fully completed claim form. This ensures that all services are accounted for.
When submitting a claim to a secondary payer, complete the entire form and attach the primary payer’s Explanation of Benefits (EOB). You can also note the amount paid by the primary carrier in the remarks field.
The NPI is a unique identifier assigned to dental providers by the federal government. It is essential for billing purposes and helps streamline the claims process. Dentists are required to include their NPI on the claim form if they are considered HIPAA covered entities.
Provider Specialty Codes indicate the type of dental professional who delivered the treatment. These codes help insurance companies understand the nature of the services provided. You should enter the appropriate code in the designated field on the claim form.
Comprehensive instructions for completing the ADA Dental Claim Form can be found in the ADA publication titled CDT-2007/2008. Additionally, updates and further resources are available on the ADA's website.
Filling out the ADA Dental Claim form can be straightforward, but there are common mistakes that can lead to delays or issues with processing. One frequent error is not marking the correct type of transaction. It's essential to check all applicable boxes for the transaction type, such as "Statement of Actual Services" or "Request for Predetermination/Preauthorization." Missing this step can result in the claim being processed incorrectly.
Another mistake is providing incomplete or inaccurate policyholder information. Ensure that the policyholder's name, address, and other details are filled out completely. Omitting a middle initial or suffix can cause confusion and may lead to claim denials.
Many people forget to include the date of birth for both the policyholder and the patient. This information is crucial for verifying coverage. Additionally, using the wrong format for dates can lead to processing issues. Always use the MM/DD/CCYY format as specified on the form.
In the section regarding other insurance coverage, individuals sometimes fail to indicate whether there is other dental or medical coverage. If "Yes" is selected, it is important to complete all relevant fields. Skipping this step can complicate the coordination of benefits.
Another common oversight is neglecting to sign the form. Both the patient and the subscriber must provide their signatures where indicated. Without these signatures, the claim may not be processed, leading to further delays.
When listing procedures, some individuals do not include all necessary details, such as the procedure date or fee. Each procedure should be clearly documented to avoid confusion. If there are more procedures than available lines on the form, a separate claim form should be used.
Lastly, failing to provide the National Provider Identifier (NPI) for the dentist can result in issues. This identifier is essential for processing claims and should be included accurately. Ensuring all sections of the form are complete and correct can help in the smooth processing of dental claims.
The ADA Dental Claim Form is an essential document for submitting dental insurance claims. Along with this form, there are several other documents that may be needed to ensure the claim is processed smoothly. Below is a list of common forms and documents that are often used in conjunction with the ADA Dental Claim Form.
Having these documents prepared can help streamline the claims process and reduce delays in receiving payment from the insurance company. It is advisable to check with the specific insurance provider for any additional requirements that may be necessary.
The ADA Dental Claim Form serves as a vital document in the dental insurance process, and several other forms share similarities with it in terms of structure and purpose. Below is a list of five documents that resemble the ADA Dental Claim Form, highlighting their similarities.
When filling out the ADA Dental Claim Form, attention to detail is crucial. Here are ten important dos and don'ts to ensure your submission is accurate and complete.
When it comes to submitting a dental claim using the ADA Dental Claim Form, several misconceptions can lead to confusion. Understanding these misconceptions can help ensure that claims are processed smoothly and efficiently. Here are eight common misunderstandings:
By addressing these misconceptions, individuals can better navigate the claims process, ensuring that all necessary information is accurately provided. This not only facilitates timely processing but also helps avoid potential issues with insurance coverage and payments.
Filling out the ADA Dental Claim Form correctly is crucial for ensuring that dental claims are processed smoothly. Here are some key takeaways to keep in mind:
By following these guidelines, you can help ensure that your dental claims are processed efficiently and accurately.