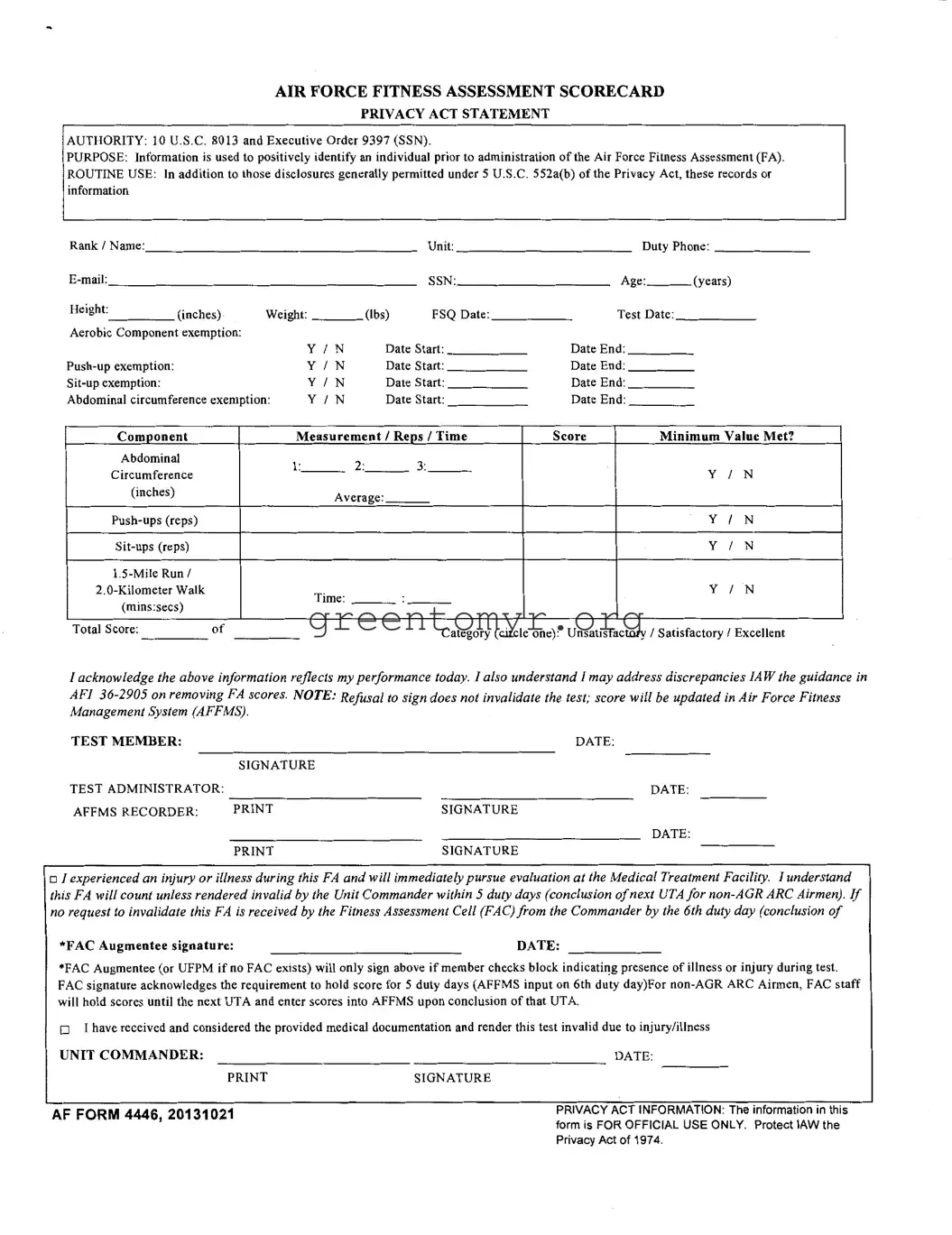
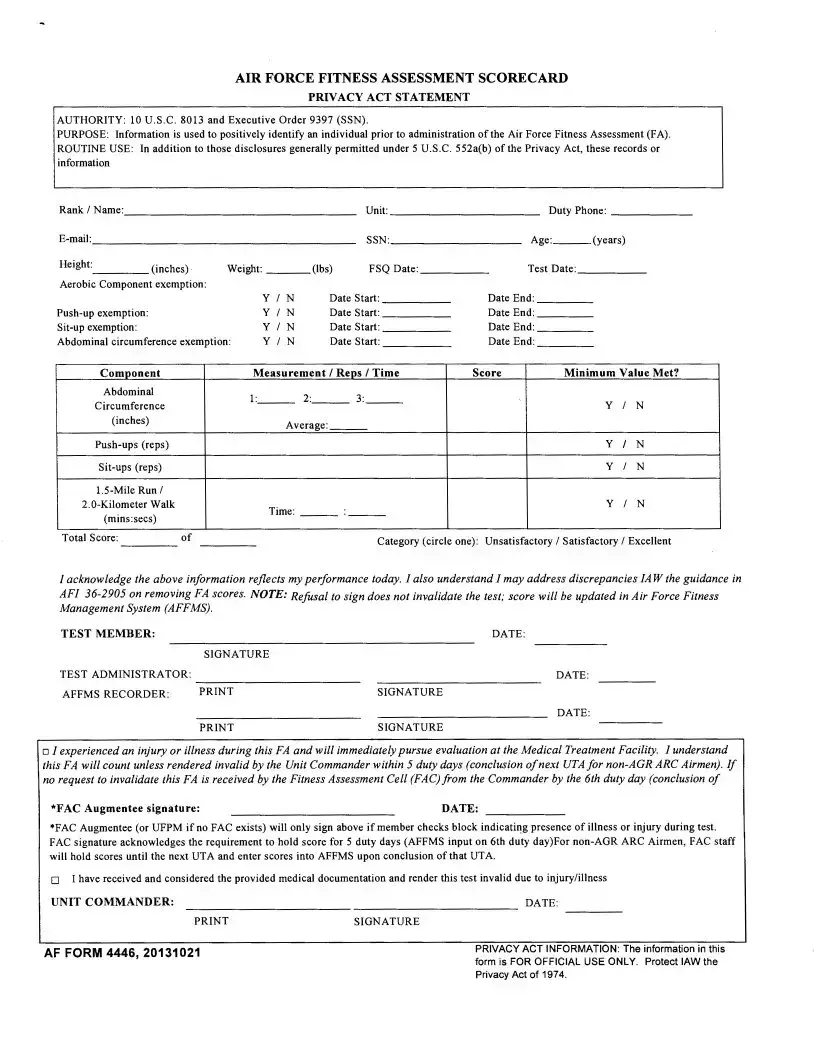
The AF 4446 form plays a crucial role in the administration of the Air Force Fitness Assessment (FA), ensuring accurate identification and documentation of individuals' fitness metrics. Designed to collect essential personal information, including rank, unit, and contact details, the form requires individuals to provide their Social Security Number, age, height, and weight. It also tracks any exemptions related to fitness components, such as aerobic capacity and strength exercises, along with the specific test scores achieved during the assessment. This scorecard documents the performance results for push-ups, sit-ups, and the timed run or walk, categorizing overall fitness as unsatisfactory, satisfactory, or excellent. Furthermore, it emphasizes the importance of acknowledging performance results, addressing any discrepancies according to Air Force instructions, and ensuring transparency by capturing signatures from the test member, administrator, and recorder. The collected data is strictly confidential and is handled per the Privacy Act, reinforcing the importance of safeguarding personal information while promoting fitness within the Air Force.
AIR FORCE FITNESS ASSESSMENT SCORECARD
PRIVACY ACT STATEMENT
AUTHORITY: 10 U.S.C. 8013 and Executive Order 9397 (SSN).
PURPOSE: Information is used to positively identify an individual prior to administration of the Air Force Fitness Assessment (FA).
ROUTINE USE: In addition to those disclosures generally permitted under 5 U.S.C. 552a(b) of the Privacy Act, these records or information
Rank/Name:._________________________________ |
Unit: |
Duty Phone: __________ |
|||||||||
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|||
Age: ___ (years) |
|
||||||||||
|
|
|
|
|
|
|
|
|
|||
Height:____ (inches) |
Weight: ___ (lbs) |
FSQ Date: _____ |
Test Date: _____ |
||||||||
Aerobic Component exemption: |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
YIN |
Date Start: ______ |
Date End: _____ |
|
|
|||
|
|
YIN |
Date Start: _____ |
Date End: _____ |
|
|
|||||
|
|
YIN |
Date Start: ______ |
Date End: _____ |
|
|
|||||
Abdominal circumference exemption: |
YIN |
Date Start: ______ |
Date End: ______ |
|
|
||||||
Component |
|
|
Measurement I Reps I Time |
Score |
|
Minimum Value Met? |
|||||
Abdominal |
|
|
1:______ |
|
|
|
|
|
|||
|
|
|
|
|
|
y |
I |
|
|||
Circumference |
|
|
|
|
|
N |
|||||
(inches) |
|
|
Average: |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
y |
I |
N |
||
|
|
|
|
|
|
|
y |
I |
N |
||
|
|
|
|
|
|
|
|
|
|
||
|
|
Time: |
|
|
y |
I |
N |
||||
(mins:secs) |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
||
Total Score: |
of |
|
|
|
Category (circle one): Unsatisfactory I Satisfactory I Excellent |
||||||
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
I acknowledge the above information reflects my performance today. I also understand I may address discrepancies !A W the guidance in
AFI
TEST MEMBER: |
|
DATE: |
|
SIGNATURE |
|
TEST ADMINISTRATOR: |
DATE: |
|
AFFMS RECORDER: |
SIGNATURE |
|
|
|
DATE: |
|
SIGNATURE |
|
o I experienced an injury or illness during this FA and will immediately pursue evaluation at the Medical Treatment Facility. I understand this FA will count unless rendered invalid by the Unit Commander within 5 duty days (conclusion ofnext UTA for
*FAC Augmentee signature: |
DATE: |
*FAC Augmentee (or UFPM if no FAC exists) will only sign above if member checks block indicating presence of illness or injury during test. FAC signature acknowledges the requirement to hold score for 5 duty days (AFFMS input on 6th duty day)For
o I have received and considered the provided medical documentation and render this test invalid due to injury/illness
UNIT COMMANDER: |
DATE: |
|
SIGNATURE |
||
AF FORM 4446, 20131021 |
PRIVACY ACT INFORMATION: The information in this |
|
form is FOR OFFICIAL USE ONLY. Protect lAW the |
||
|
||
|
Privacy Act of 1974. |
| Fact Name | Description |
|---|---|
| Form Purpose | The AF 4446 form serves to identify individuals before their Air Force Fitness Assessment. |
| Governing Authority | It is governed by 10 U.S.C. 8013 and Executive Order 9397 (related to SSNs). |
| Privacy Protection | This form is handled in accordance with the Privacy Act of 1974, ensuring confidentiality. |
| Information Required | Personal information collected includes rank, name, unit, duty phone, email, age, height, weight, and SSN. |
| Health Exemptions | Exemptions for various components of the fitness assessment can be documented, including push-ups and sit-ups. |
| Fitness Scores | The form captures scores for multiple components, including push-ups, sit-ups, and the 1.5-mile run. |
| Assessment Categories | Participants can receive ratings of Unsatisfactory, Satisfactory, or Excellent based on their scores. |
| Signature Requirement | Participants must acknowledge their performance by signing the form, alongside the test administrator. |
| Medical Concerns | There are provisions for addressing injuries or illnesses that occur during the assessment. |
| Record Management | The scores and related information are managed in the Air Force Fitness Management System (AFFMS). |
Filling out the AF 4446 form is a straightforward process that requires accurate personal information and performance details. After completing this form, submit it to the appropriate personnel for processing. Ensure all sections are filled out carefully to avoid any delays.
The AF 4446 form, also known as the Air Force Fitness Assessment Scorecard, serves several important functions. Its primary purpose is to collect essential information about an individual prior to administering the Air Force Fitness Assessment (FA). This includes personal details like rank, name, unit, and contact information which are needed to accurately identify and record each member's performance. Additionally, the form includes exemptions for different fitness components, ensuring that individual circumstances are considered. Protecting privacy is paramount, and the information gathered is handled according to the Privacy Act of 1974.
The AF 4446 form requires a range of personal details to effectively document your fitness assessment. Key information includes:
Collecting this information helps in creating an accurate scorecard and ensures personalized considerations are made for fitness assessments.
If you experience an injury or illness during the fitness assessment, it is crucial to indicate this on the AF 4446 form. In this case, you must seek evaluation at a Medical Treatment Facility. Your fitness score will still be logged but can be deemed invalid if your Unit Commander submits a request within 5 duty days for that assessment to be invalidated. If the request isn't received within that timeframe, the score will be officially recorded in the Air Force Fitness Management System (AFFMS).
The information collected through the AF 4446 form is treated with the utmost confidentiality. It is classified as "FOR OFFICIAL USE ONLY," indicating that it should be used solely for its intended purpose. The guidelines set forth in the Privacy Act of 1974 govern the collection, maintenance, and dissemination of personal information, helping to ensure that individuals' details remain secure and protected. Individuals are encouraged to be aware of these protections when filling out the form.
Signing the AF 4446 form is a critical step in the process of the fitness assessment. By signing, you acknowledge that the information recorded accurately reflects your performance on the day of the assessment. If discrepancies arise, these can be addressed following the guidance in AFI 36-2905, which outlines processes for contesting fitness scores. Furthermore, refusing to sign does not invalidate the test; the score will still be updated in the AFFMS, but your acknowledgment is important for record-keeping and transparency.
When filling out the AF 4446 form, many individuals make common mistakes that can lead to complications. One prevalent error is failing to enter accurate personal details. The section asking for rank, name, unit, and contact information must be filled out correctly. Omissions can delay processing or hinder identification during the fitness assessment.
Another mistake is neglecting to specify exemptions for the aerobic component or various exercises. If applicable, an absence of dates or incorrect markings in these sections can result in confusion. Participants should ensure they indicate whether an exemption is claimed and provide the corresponding start and end dates.
Some people incorrectly mark their scores or measurements. The area for recording the abdominal circumference, push-up, sit-up, and run/walk times requires precision. Errors in these figures not only affect the overall score but also the assessments made by superiors.
Moreover, failing to sign or date relevant sections of the form can render it incomplete. The signatures of both the test member and the test administrator are necessary. A missing signature can cause issues with recordkeeping and the enforcement of any decisions related to the fitness assessment.
Another common issue arises with the acknowledgment of injuries or illnesses. Participants must check the box indicating they experienced an injury and pursue the necessary evaluation. Skipping this step can lead to scores being counted when they should be invalid, potentially affecting a member's fitness record.
Individuals sometimes misunderstand the timeline for submitting requests to invalidate a score. If the unit commander fails to act within 5 duty days, the score remains valid. Awareness of these deadlines is crucial to prevent unintended consequences.
It's also essential to ensure that the total score and category selection are accurately reported. An incorrect total score can misrepresent performance, leading to disciplinary action. Participants should double-check their calculations before submission.
Finally, disregarding the Privacy Act statement can lead to improper handling of sensitive information. Participants must understand the confidentiality of the provided data and ensure it is protected according to regulations.
The AF 4446 form, known as the Air Force Fitness Assessment Scorecard, plays a significant role in documenting the fitness performance of Air Force personnel. Alongside this form, several other documents are frequently used to ensure a comprehensive approach to fitness assessment and personnel management. The following are six important forms and documents commonly associated with the AF 4446:
Utilizing these documents in conjunction with the AF 4446 ensures a thorough evaluation of physical fitness and adherence to required standards. Keeping accurate records supports the overall health and readiness of Air Force personnel.
The AF 4446 form, known as the Air Force Fitness Assessment Scorecard, serves as an essential document for tracking fitness assessments within the Air Force. Several other documents share similarities with the AF 4446 form in terms of purpose, information collection, and the importance they hold in monitoring fitness or health-related requirements. Below is a list of eight such documents.
These documents share a focus on health, fitness standards, and the collection of personal information necessary for effective oversight and management within military environments. Each of them plays a role in ensuring that military personnel meet the demands of their roles, emphasizing the importance of fitness and health assessments.
When filling out the AF 4446 form, it is important to follow certain guidelines to ensure accuracy and compliance. Here are ten things to keep in mind:
Understanding the AF 4446 form is crucial for those involved in the Air Force Fitness Assessment process. However, several misconceptions about this form can lead to confusion and misinformation. Here are five common misconceptions:
By addressing these misconceptions, Air Force personnel can better understand the AF 4446 form's significance and requirements.