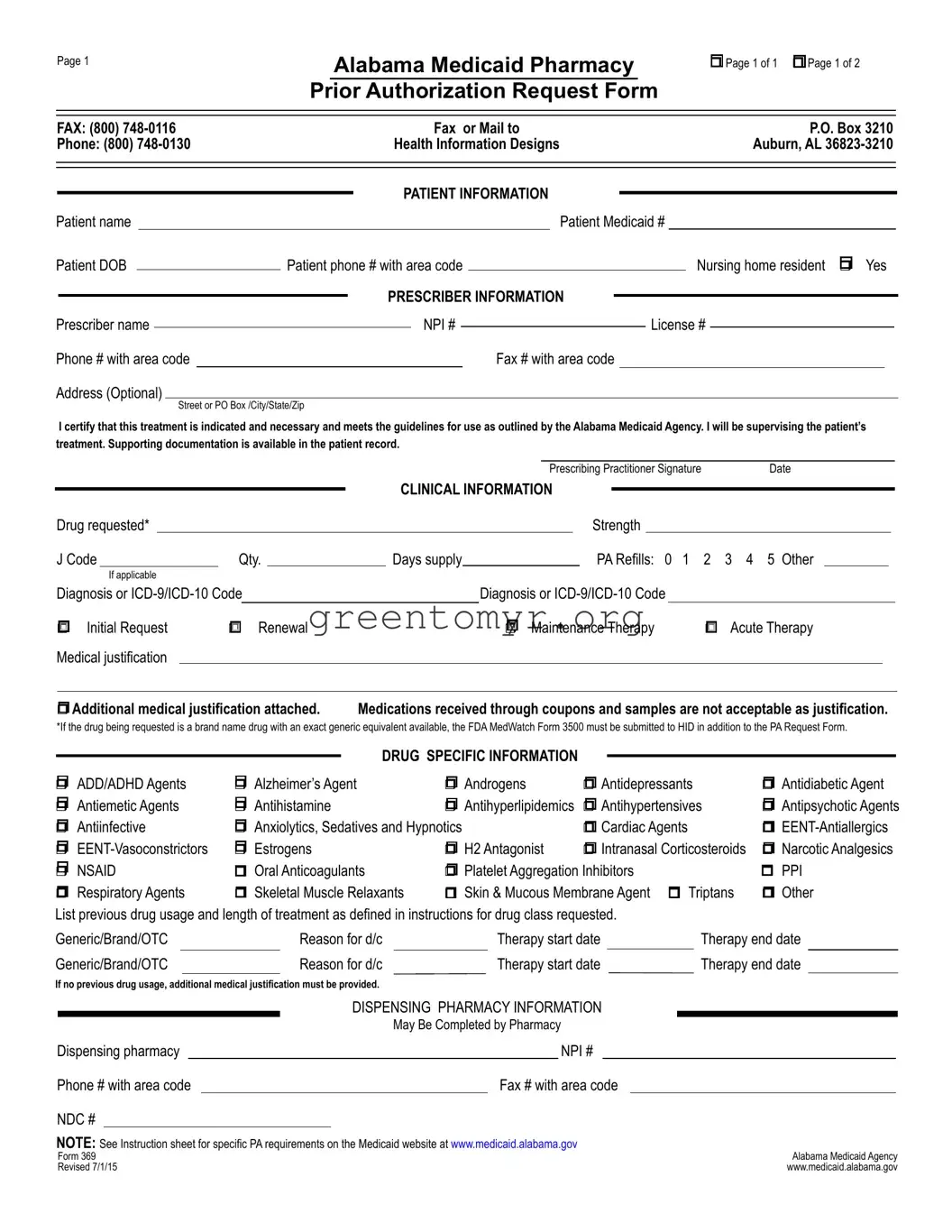
The Alabama 369 form, officially known as the Alabama Medicaid Pharmacy Prior Authorization Request Form, is a critical document designed to facilitate the approval process for specific medications under the state's Medicaid program. This form serves as a comprehensive tool for healthcare providers to submit detailed information regarding a patient's medication needs. Key sections of the form include patient information, prescriber details, clinical information about the requested drug, and dispensing pharmacy data. Each section is meticulously structured to capture essential data, such as the patient's Medicaid number, diagnosis codes, and prior medication usage. In addition, healthcare professionals must provide medical justifications for the requested drugs, indicating whether the request is for an initial approval, renewal, or maintenance therapy. Special attention is given to certain drug categories, allowing prescribers to specify the class of medication being requested, ranging from antidepressants to antidiabetics, ensuring that both clinical need and adherence to established guidelines are explicitly stated. The form also addresses unique circumstances, such as prior authorization requirements for medications with generic equivalents or specific protocols for pediatric patients. Ultimately, the Alabama 369 form plays a vital role in managing patient care effectively while ensuring compliance with Medicaid regulations.

Page 1
Alabama Medicaid Pharmacy
Prior Authorization Request Form
rPage 1 of 1 r Page 1 of 2
FAX: (800) |
|
|
|
Fax or Mail to |
|
|
|
|
P.O. Box 3210 |
|
|||||||||||||
Phone: (800) |
|
|
Health Information Designs |
|
|
|
|
Auburn, AL |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Patient name |
|
|
|
|
|
|
|
|
Patient Medicaid # |
|
|
||||||||||||
Patient DOB |
|
|
Patient phone # with area code |
|
|
|
|
Nursing home resident r Yes |
|
||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
PRESCRIBER INFORMATION |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Prescriber name |
|
|
|
|
|
|
NPI # |
|
|
|
|
License # |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Phone # with area code |
|
|
|
|
|
|
Fax # with area code |
|
|
|
|
|
|
|
|
||||||||
Address (Optional) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
I certify that this treatment is indicated and necessary and meets the guidelines for use as outlined by the Alabama Medicaid Agency. I will be supervising the patient’s treatment. Supporting documentation is available in the patient record.
|
|
|
|
|
|
|
|
|
|
|
|
|
Prescribing Practitioner Signature |
Date |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CLINICAL INFORMATION |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Drug requested* |
|
|
|
|
|
|
|
|
|
|
|
Strength |
|
|
|
|
|
|
|
||||
|
J Code |
Qty. |
|
Days supply |
|
|
|
PA Refills: 0 1 |
2 3 4 5 Other |
|
||||||||||||||
|
|
If applicable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Diagnosis or |
|
|
|
Diagnosis or |
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
r Initial Request |
r Renewal |
|
|
|
r |
Maintenance Therapy |
r Acute Therapy |
|
|||||||||||||||
|
Medical justification |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
r Additional medical justification attached. |
Medications received through coupons and samples are not acceptable as justification. |
|
|||||||||||||||||||||
*If the drug being requested is a brand name drug with an exact generic equivalent available, the FDA MedWatch Form 3500 must be submitted to HID in addition to the PA Request Form.
|
|
|
|
|
|
|
|
|
|
DRUG SPECIFIC INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
||
r ADD/ADHD Agents |
r Alzheimer’s Agent |
r Androgens |
r Antidepressants |
r Antidiabetic Agent |
|||
r Antiemetic Agents |
r Antihistamine |
r Antihyperlipidemics |
r Antihypertensives |
r Antipsychotic Agents |
|||
r Antiinfective |
r Anxiolytics, Sedatives and Hypnotics |
r Cardiac Agents |
r |
||||
r |
r Estrogens |
r H2 Antagonist |
r Intranasal Corticosteroids |
r Narcotic Analgesics |
|||
r NSAID |
r Oral Anticoagulants |
r Platelet Aggregation Inhibitors |
r PPI |
||||
r Respiratory Agents |
r Skeletal Muscle Relaxants |
r Skin & Mucous Membrane Agent r Triptans |
r Other |
||||
List previous drug usage and length of treatment as defined in instructions for drug class requested. |
|
|
|
|
||||||||||||||
Generic/Brand/OTC |
|
Reason for d/c |
|
Therapy start date |
|
|
Therapy end date |
|
||||||||||
Generic/Brand/OTC |
|
Reason for d/c |
|
Therapy start date |
|
Therapy end date |
|
|||||||||||
If no previous drug usage, additional medical justification must be provided. |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DISPENSING PHARMACY INFORMATION |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
May Be Completed by Pharmacy |
|
|
|
|
|||||
Dispensing pharmacy |
|
|
|
|
|
NPI # |
|
|
|
|
|
|||||||
Phone # with area code |
|
|
|
|
Fax # with area code |
|
|
|
|
|
||||||||
NDC # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
NOTE: See Instruction sheet for specific PA requirements on the Medicaid website at www.medicaid.alabama.gov |
|
Alabama Medicaid Agency |
||||||||||||||||
Form 369 |
|
|
|
|
|
|
|
|
|
|||||||||
Revised 7/1/15 |
|
|
|
|
|
|
|
|
|
www.medicaid.alabama.gov |
||||||||
Page 2 |
Patient Medicaid # |
rSustained Release Oral Opioid Agonist
Proposed duration of therapy |
|
|
|
|
Is medicine for PRN use? |
r Yes |
r No |
|
|||
Type of pain r Acute r Chronic |
|
|
|
Severity of pain: r Mild |
r Moderate r Severe |
|
|||||
Is there a history of substance abuse or addiction? r Yes |
r No |
|
|
|
|||||||
If yes, is treatment plan attached? |
r Yes r No |
|
|
|
|
|
|
|
|
||
Indicate prior and/or current analgesic therapy and alternative management choices |
|
|
|
||||||||
Drug/therapy |
|
|
|
|
Reason for d/c |
|
|
|
|
|
|
Drug/therapy |
|
|
|
Reason for d/c |
|
|
|
|
|||
|
|
|
|
|
|||||||
r Antipsychotic Agents |
The request is for: |
r Monotherapy or r Polytherapy |
|
|
|||||||
For children < 6 years of age, have monitoring protocols (see Attachment C on the Alabama Medicaid website) been followed? r Yes r No For polytherapy and/or
Medical justification may include peer reviewed literature, medical record documentation, chart notes with specific symptoms that the support the diagnosis, etc.
rXenicalR
r |
If initial request |
Weight |
|
kg. |
|
Height |
|
inches |
BMI |
|
|
kg/m2 |
|||
r |
If renewal request |
Previous weight |
|
|
|
kg. |
Current weight |
|
|
|
kg. |
|
|
||
Documentation MD supervised exercise/diet regimen > 6 mo.? r Yes |
r No |
Planned adjunctive therapy? r Yes |
r No |
||||||||||||
r Phosphodiesterase Inhibitors |
|
|
|
|
|
|
|
|
||
Failure or inadequate response to the following alternate therapies: |
|
|
|
|
|
|||||
1. |
|
|
|
2. |
|
|
3. |
|
|
|
4. |
|
|
|
5. |
|
|
6. |
|
|
|
Contraindication of alternate therapies: |
|
|
|
|
|
|
|
|
||
r Documentation of vasoreactivity test attached |
r Consultation with specialist attached |
|
|
|||||||
|
|
|
|
|
|
|||||
r Specialized Nutritionals |
Height |
inches |
Current weight |
kg. |
|
|||||
rIf < 21 years of age, record supports that > 50% of need is met by specialized nutrition
rIf > 21 years of age, record supports 100% of need is met by specialized nutrition
Method of administration |
|
Duration |
|
|
|
|
# of refills |
|||
|
|
|
|
|
|
|
|
|
|
|
r Xolair® |
Current Weight:__________kg (patient’s weight must be between |
|||||||||
Is the patient 12 years or older? |
|
|
|
r |
Yes |
r |
No |
|||
Is the request for chronic idiopathic urticaria? |
r |
Yes |
r |
No |
||||||
Is the request for moderate to severe asthma and is treatment recommended by a board |
|
|
|
|
|
|
|
|||
certified pulmonologist or allergist after their evaluation (if yes answers questions below)? |
r |
Yes |
r |
No |
||||||
Has the patient had a positive skin or blood test reaction to a perennial aeroallergen? |
r |
Yes |
r |
No |
||||||
Is the patient symptomatic despite receiving a combination of either inhaled corticosteroid |
|
|
|
|
|
|
|
|||
and a leukotriene inhibitor or an inhaled corticosteroid and long acting beta agonist or has |
|
|
|
|
|
|
|
|||
the patient required 3 or more bursts of oral steroids within the past 12 months? |
r |
Yes |
r |
No |
||||||
Are the patient’s baseline IgE levels between 30 IU/mL and 700 IU/mL? |
r |
Yes |
r |
No |
||||||
Level:_________________ |
Date:__________________ |
|
|
|
|
|
|
|
||
Form 369 |
Alabama Medicaid Agency |
Revised |
www.medicaid.alabama.gov |
| Fact Name | Description |
|---|---|
| Form Purpose | The Alabama 369 form is used for requesting prior authorization for medications through Alabama Medicaid. |
| Governing Law | This form operates under the Alabama Medicaid Agency guidelines. |
| Patient Information Required | Key patient details needed include name, Medicaid number, date of birth, and phone number. |
| Prescriber Information | Prescribers must provide their name, NPI number, and license number, among other contact details. |
| Drug Information | Information about the requested drug includes its name, strength, and quantity needed. |
| Clinical Purpose | The form distinguishes between initial requests, renewals, maintenance, and acute therapy. |
| Documentation Requirement | Supporting medical justification must be attached if necessary and must comply with Medicaid regulations. |
| Pharmacy Information | Dispensing pharmacy details, such as name, NPI, and phone number, should be included, if applicable. |
| Substance Abuse Question | The form includes questions regarding the patient's history of substance abuse or addiction. |
| Revisions Date | The Alabama Medicaid 369 form was last revised on July 1, 2015. |
Filling out the Alabama 369 form is a critical step in obtaining prior authorization for certain medications through the Alabama Medicaid program. This form requires detailed patient, prescriber, and drug information. Ensure all sections are completed accurately to avoid any delays in processing your request.
The Alabama 369 form is a Pharmacy Prior Authorization Request form used by healthcare providers to request medication coverage through Alabama Medicaid. It is essential for obtaining approval for specific medications, especially those that require prior authorization due to cost or clinical necessity.
The form should be completed by the prescribing healthcare provider. This could be a physician, nurse practitioner, or any medical professional authorized to prescribe medication. The prescriber must ensure that all necessary details regarding the patient and the medication are accurately represented on the form.
The Alabama 369 form requests several details:
After filling out the form, you can submit it through fax or mail. The fax number is (800) 748-0116, and the mailing address is:
P.O. Box 3210, Auburn, AL 36823-3210. For questions, you can call (800) 748-0130.
There are various categories of medications that may require prior authorization. These include:
Before prescribing, healthcare providers should verify if the medication requires prior authorization to avoid delays in treatment.
If the requested medication has a generic equivalent available, the FDA MedWatch Form 3500 must be submitted along with the Alabama 369 form. This requirement helps ensure that patients are receiving the most cost-effective treatment options.
The prescriber must include medical justification for the requested medication. This can be in the form of medical records, notes detailing specific symptoms, or any peer-reviewed literature supporting the request. If medications were previously received through coupons or samples, this will not be accepted as justification.
The processing time for prior authorization requests can vary. Typically, healthcare providers can expect a response within a few days after submission. However, urgent requests may be expedited, while incomplete forms could delay the process.
Filling out the Alabama 369 form can be straightforward if you pay attention to details. However, many individuals make common mistakes that can hinder the approval process for medication. Here are some of the most frequent errors.
One mistake frequently made is not providing accurate patient information. This includes the patient's name, Medicaid number, and date of birth. Inaccuracies can lead to delays or outright denials. Ensure that all details are current and match what's on file with Medicaid.
An incomplete prescriber section can also create problems. Each prescriber must include their name, NPI number, and license number, among other details. Omitting this information can slow down the processing time. Fill in all required fields thoroughly to expedite the review process.
Medical justification is an essential part of the form. Some individuals underestimate its importance and fail to provide sufficient supporting documentation. If medical justification is lacking, the request may be rejected. Always attach any additional documentation that will substantiate the need for the medication.
Not checking the drug-specific information section is another common error. Each drug requested must align with specific categories, and a lack of attention here may result in confusion or rejection. Take the time to check the boxes that correctly correspond to the medication being requested.
Another area of concern involves previous medications. If patients have used alternative therapies, they need to detail their history accurately. Leaving out information about prior medications can make it seem like alternative treatments were never tried, which is often a requirement for approval.
Additionally, some users neglect to verify if previous drug usage requires additional medical justification when no prior medications have been documented. This oversight can lead to rejection because the reviewer may deem the request as unsupported.
It’s crucial to also ensure that the form is signed and dated correctly. A missing signature or date can render the entire form invalid. Always double-check this before submission.
Lastly, many individuals submit the form without properly reviewing the fax or mailing instructions. Each submission method has specific requirements. Make sure to follow the guidelines closely to avoid unnecessary delays.
By addressing these common mistakes, those filling out the Alabama 369 form can improve their chances of successful medication approval. Attention to detail can make a significant difference in the pharmacy prior authorization process.
The Alabama 369 form is an essential document used for prior authorization requests in the context of Medicaid pharmacy services. Its purpose is to gather necessary information about the patient, the prescriber, and the drug being requested. In addition to the Alabama 369 form, several other documents are frequently used in conjunction with it to ensure a comprehensive review and approval process. Below is a list of these documents, along with a brief description of each.
Utilizing these forms and documents alongside the Alabama 369 form helps create a robust case for prior authorization requests. This comprehensive approach not only supports the approval process but also reinforces the commitment to ensuring that patients receive the necessary medications for their health needs. Clear and accurate documentation is vital in navigating the complexities of the healthcare system, ultimately leading to better patient outcomes.
Prior Authorization Request Form (PAR): Like the Alabama 369 form, the Prior Authorization Request Form serves to obtain permission from a healthcare insurer before specific treatments or medications are provided. This ensures the requested treatment aligns with the insurance provider's coverage policies.
Drug Utilization Review (DUR) Form: Similar to the Alabama 369 form, a DUR form assesses the appropriateness of prescribed medications. It reviews factors like potential drug interactions, duplications, and therapeutic duplications, aiming for optimal patient safety.
Medicaid Prescription Drug Request Form: This document parallels the Alabama 369 form by enabling healthcare providers to request specific drugs for their patients. It focuses on adherence to Medicaid's requirements for coverage and documentation.
Specialty Medication Authorization Form: Just like the Alabama 369, this form is necessary for patient access to high-cost specialty medications. It usually requests detailed clinical information to justify the need for these specialized treatments.
Medicare Part D Exception Request Form: Similar to the Alabama 369 form, this document enables healthcare providers to request exceptions for drugs not typically covered under Medicare Part D plans. Justification is required to demonstrate medical necessity.
Clinical Trial Enrollment Form: This form shares similarities with the Alabama 369 by collecting clinical details to assess eligibility for participation in a clinical trial. It gathers patient history and other relevant medical information to ensure compliance with the study criteria.
When filling out the Alabama 369 form, it's crucial to adhere to proper guidelines to ensure your request is processed efficiently. Below are four important do's and don'ts to keep in mind.
This form is not limited to initial requests. It can also be utilized for renewing existing medications or for maintenance therapy. Individuals and prescribers should understand that the form serves multiple purposes in the authorization process.
Approval is not automatic upon submission. Each request undergoes a review process based on medical necessity and adherence to guidelines defined by the Alabama Medicaid Agency. It's important for prescribers to include thorough justifications to enhance the chances of approval.
Not every medication falls under the need for a prior authorization. Some medications, especially generics or those deemed essential, may not require this step. It is advisable to review the guidelines or consult with a pharmacy for clarity.
In many cases, comprehensive documentation is essential. This may include clinical rationale, previous treatment history, and details regarding the patient’s medical condition. The completeness of documentation significantly impacts the success of the authorization request.
Patients and prescribers can inquire about the status of their prior authorization request after submission. Communication lines are open, allowing them to follow up and address any additional requirements that may arise during the review process.
When filling out and utilizing the Alabama 369 Form for Medicaid Pharmacy Prior Authorization, it’s crucial to keep the following points in mind:
Filling out the Alabama 369 Form accurately and thoroughly can streamline the approval process. Missing information can lead to delays, so be diligent and proactive when submitting this important request.