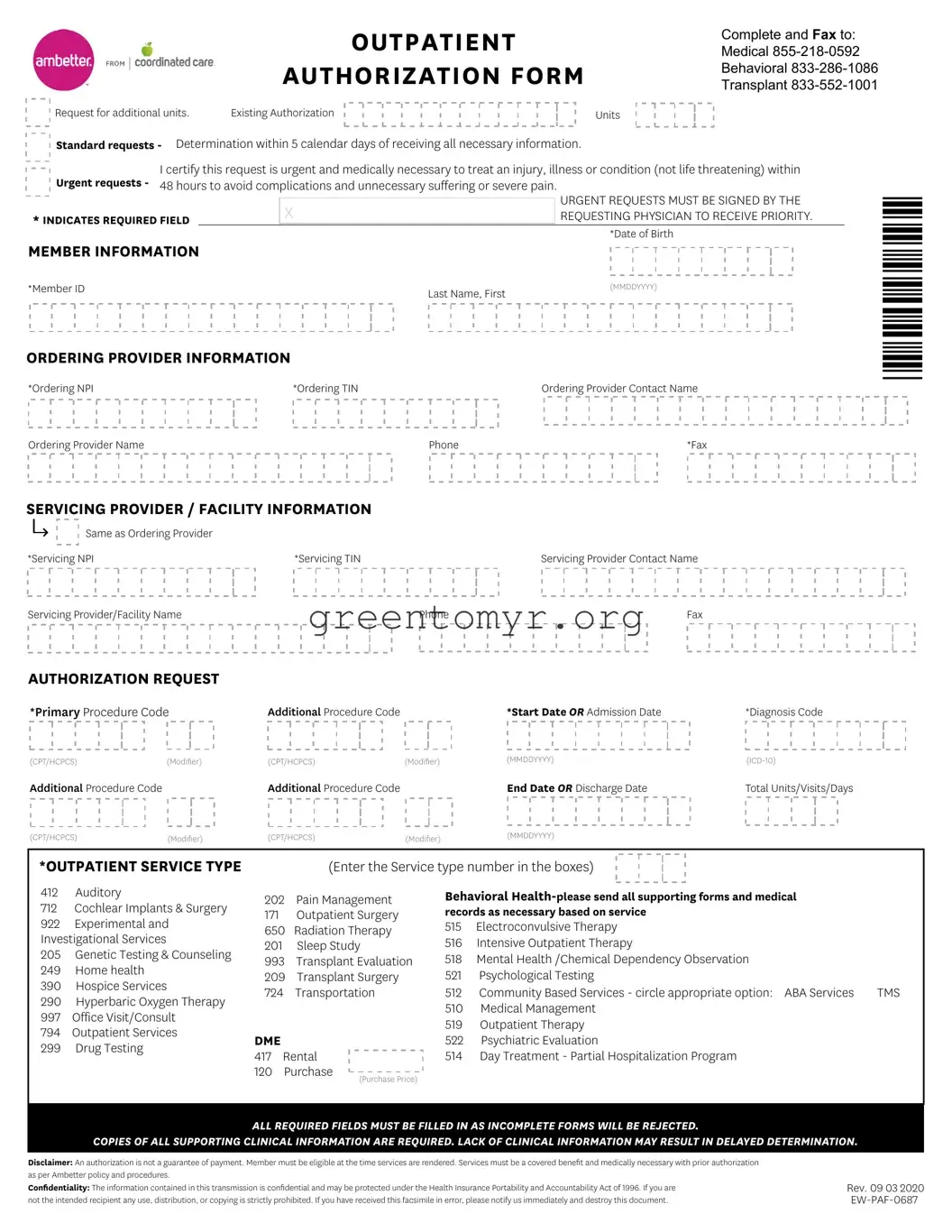
The Ambetter Outpatient Authorization Form serves as a crucial step in the process of obtaining medical services and treatments for patients enrolled in Ambetter coverage. Designed for both standard and urgent requests, this form lays out specific requirements for healthcare providers, ensuring that authorization is granted in a timely manner. For standard requests, anticipate a determination within five calendar days, while urgent requests can prompt a quicker response if certified as medically necessary. Clearly marked required fields, including member ID and ordering provider details, must be completed to avoid rejections due to incomplete submissions. The form captures multiple aspects of the requested services, including procedure codes, diagnosis codes, and specific service types ranging from outpatient surgeries to behavioral health services. Given the complexity of healthcare billing and service authorization, it’s vital to include all necessary clinical information, as gaps can lead to delays. Additionally, it is important to understand that authorization does not guarantee payment; careful attention to compliance with coverage guidelines is essential to ensure eligibility and benefits for the care provided.
OUTPATIENT
AUTHORIZATION FORM
Complete and Fax to: Medical
Request for additional units. |
Existing Authorization |
Units
Standard requests - Determination within 5 calendar days of receiving all necessary information.
Urgent requests - |
I certify this request is urgent and medically necessary to treat an injury, illness or condition (not life threatening) within |
|||||
48 hours to avoid complications and unnecessary suffering or severe pain. |
||||||
|
|
|
|
|
|
URGENT REQUESTS MUST BE SIGNED BY THE |
|
|
|
X |
|
|
|
* INDICATES REQUIRED FIELD |
|
|
|
REQUESTING PHYSICIAN TO RECEIVE PRIORITY. |
||
|
|
|
|
*Date of Birth |
||
MEMBER INFORMATION |
|
|
|
|||
|
|
|
|
|||
*Member ID |
|
|
|
Last Name, First |
|
(MMDDYYYY) |
|
|
|
|
|
|
|
ORDERING PROVIDER INFORMATION |
|
|
|
|||
*Ordering NPI |
|
|
*Ordering TIN |
|
Ordering Provider Contact Name |
|
Ordering Provider Name |
|
|
|
Phone |
|
*Fax |
*0687*
SERVICING PROVIDER / FACILITY INFORMATION
Same as Ordering Provider |
|
|
*Servicing NPI |
*Servicing TIN |
Servicing Provider Contact Name |
Servicing Provider/Facility Name |
Phone |
Fax |
AUTHORIZATION REQUEST
*Primary Procedure Code |
Additional Procedure Code |
|
*Start Date OR Admission Date |
*Diagnosis Code |
|
(CPT/HCPCS) |
(Modifier) |
(CPT/HCPCS) |
(Modifier) |
(MMDDYYYY) |
|
Additional Procedure Code |
|
Additional Procedure Code |
|
End Date OR Discharge Date |
Total Units/Visits/Days |
(CPT/HCPCS) |
(Modifier) |
(CPT/HCPCS) |
(Modifier) |
(MMDDYYYY) |
|
*OUTPATIENT SERVICE TYPE
(Enter the Service type number in the boxes)
412 Auditory
712Cochlear Implants & Surgery
922Experimental and Investigational Services
205Genetic Testing & Counseling
249Home health
390Hospice Services
290Hyperbaric Oxygen Therapy
997Office Visit/Consult
794Outpatient Services
299Drug Testing
202Pain Management
171Outpatient Surgery
650Radiation Therapy
201Sleep Study
993Transplant Evaluation
209Transplant Surgery
724Transportation
DME |
|
|
417 |
Rental |
|
120 |
Purchase |
(Purchase Price) |
|
|
Behavioral
515Electroconvulsive Therapy
516Intensive Outpatient Therapy
518Mental Health /Chemical Dependency Observation
521Psychological Testing
512 |
Community Based Services - circle appropriate option: ABA Services |
TMS |
510 |
Medical Management |
|
519 |
Outpatient Therapy |
|
522 Psychiatric Evaluation |
|
|
514 |
Day Treatment - Partial Hospitalization Program |
|
ALL REQUIRED FIELDS MUST BE FILLED IN AS INCOMPLETE FORMS WILL BE REJECTED.
COPIES OF ALL SUPPORTING CLINICAL INFORMATION ARE REQUIRED. LACK OF CLINICAL INFORMATION MAY RESULT IN DELAYED DETERMINATION.
Disclaimer: An authorization is not a guarantee of payment. Member must be eligible at the time services are rendered. Services must be a covered benefit and medically necessary with prior authorization as per Ambetter policy and procedures.
Confidentiality: The information contained in this transmission is confidential and may be protected under the Health Insurance Portability and Accountability Act of 1996. If you are not the intended recipient any use, distribution, or copying is strictly prohibited. If you have received this facsimile in error, please notify us immediately and destroy this document.
Rev. 09 03 2020
| Fact Name | Description |
|---|---|
| Fax Numbers | The Ambetter Outpatient Authorization Form must be completed and faxed to the appropriate numbers: Medical at 855-218-0592, Behavioral at 833-286-1086, and Transplant at 833-552-1001. |
| Urgent Request Criteria | For urgent requests, the request must be certified as urgent and medically necessary to treat a condition within 48 hours. This is crucial to avoid complications and unnecessary suffering. |
| Required Fields | To ensure the application is processed without delay, every required field on the form must be filled in completely. Incomplete submissions will be rejected. |
| Supporting Information | Copies of all supporting clinical information are mandatory with the submission. Insufficient clinical details may lead to delayed determinations for authorization. |
| Confidentiality Notice | The information in the submission is confidential and may be protected under the Health Insurance Portability and Accountability Act (HIPAA) of 1996. Unauthorized use or distribution is prohibited. |
Filling out the Ambetter Out Patient form is a straightforward process that ensures the necessary information for authorization is collected. It's important to carefully complete each section to avoid any delays in processing your request.
Once the form is submitted, it will undergo review, and you will receive a determination within the stated time frame. Make sure to keep track of any additional information that may be requested to ensure a smooth process.
The Ambetter Out Patient form is used to request prior authorization for outpatient services. This includes services like outpatient surgery, mental health treatments, and other medical procedures. Completing this form helps ensure that the requested services are medically necessary and covered by your Ambetter insurance plan.
After completing the form, fax it to the appropriate number based on the type of service being requested. Here are the numbers:
Make sure to send your form to the correct number to avoid delays in processing your request.
You must fill out several fields on the Ambetter Out Patient form. Key information includes:
It's essential to complete all required fields. Incomplete forms will be rejected.
Urgent requests are for services that are medically necessary but not life-threatening. These requests must be submitted with urgency certification and can be processed within 48 hours. You need to sign the form to indicate that it is an urgent request. Be sure to specify that it’s urgent and fill in the necessary fields to avoid delays.
No, submitting the Ambetter Out Patient form does not guarantee payment. Payment depends on member eligibility at the time services are provided. Services must also be considered a covered benefit and medically necessary according to Ambetter policies. It’s important to check your plan details to understand coverage requirements.
Correctly completing the Ambetter Out Patient form is crucial for efficient processing of medical requests. Many people encounter issues that can lead to delays or even rejections of their submissions. Here are eight common mistakes to avoid when filling out the form.
First, many individuals overlook the required fields. Every section marked with an asterisk (*) must be filled out. Omitting even one of these fields can result in the entire form being deemed incomplete, leading to rejection. Careful attention to these details will help facilitate a smoother authorization process.
Another frequent error is incorrectly entering the member’s information. The Member ID, last name, and first name should be accurately entered as they appear on the member’s insurance card. Double-checking these entries ensures that the request is easily matched with the member's file.
People often neglect to provide complete ordering provider information. This includes the Ordering NPI (National Provider Identifier) and TIN (Tax Identification Number) along with the provider's name and contact details. Incomplete information can create hurdles in verifying the provider's credentials, delaying authorization.
In many instances, individuals select the incorrect service type on the form. Each service type has a specific code that allows for proper categorization of the request. Ensuring that the correct service type number is entered guarantees that the request is processed under the right guidelines.
Another mistake made is not specifying the diagnosis code properly. The form requires accurate ICD-10 codes to substantiate the medical necessity of the requested services. Inaccurate codes can lead to misunderstandings about the patient’s condition and can impede approval.
Some individuals fail to include the necessary supporting documentation. The form clearly states that copies of all clinical information are mandatory. Without these, the request may experience significant delays, as the review team cannot make an informed decision about the authorization.
Moreover, people sometimes do not check if the services are a covered benefit under the member’s plan. Familiarizing oneself with the coverage details can prevent surprises down the line, ensuring that the requested services align with their insurance policy.
Finally, many individuals overlook the importance of signing the form when submitting urgent requests. An unsigned urgent request will not be processed, even if it clearly indicates a need for rapid response. This oversight can result in unnecessary delays in patient care.
By being aware of these common pitfalls and taking the time to fill out the Ambetter Out Patient form carefully, individuals can improve their chances of timely and efficient authorization for medical services.
The Ambetter Out Patient form plays an important role in the authorization process for outpatient services. Alongside this form, several other documents are often utilized to ensure a comprehensive and efficient submission. Below is a list of related documents that may accompany the Ambetter Out Patient form.
These documents, in conjunction with the Ambetter Out Patient form, facilitate a smoother authorization process for necessary outpatient services. Ensuring that each document is complete and accurate can significantly reduce the chances of delays in obtaining approval for care.
Prior Authorization Form: This document requests approval from an insurance company before a service or procedure. Like the Ambetter Outpatient form, it requires specific patient information and details about the procedure.
Referral Form: A referral form is sent by a primary care physician to a specialist, similar to how the Ambetter Outpatient form is used to get referrals for additional services. Both require patient and provider information.
Claims Submission Form: This form submits a request for payment from the insurance company for services provided. While the Ambetter Outpatient form requests pre-approval, both documents require diagnosis and procedure codes.
Medicare Home Health Certification: This document certifies that a patient qualifies for home health services. It shares similarities in requiring patient information and identifies the types of medical services needed.
Continuity of Care Document (CCD): The CCD provides a summary of patient information and treatments received. It parallels the Ambetter Outpatient form in that both are used to communicate important patient healthcare details.
Insurance Enrollment Form: This is submitted to enroll a patient into an insurance plan. Like the Ambetter form, it collects vital information about the patient and their healthcare needs.
When filling out the Ambetter Outpatient Authorization Form, there are key actions to consider that can either facilitate or hinder the process.
The form is not optional; it is required to request prior authorization for outpatient services. Proper completion is essential for your request to be processed.
Requests fall into two categories: standard and urgent. Standard requests take up to 5 days, while urgent requests must be certified and are addressed within 48 hours.
All required fields must be filled out. Incomplete forms can lead to rejection, regardless of additional information provided.
You must include copies of all supporting clinical information. Without this, there may be delays in determining your request.
Authorization does not guarantee payment. You must be eligible for services at the time they are provided, and they must be covered benefits.
It’s important to review the form for completeness and accuracy before faxing it to avoid delays or rejections.
You must specify the outpatient service type by entering the corresponding number in the provided boxes.
The requesting physician should fill out the form to ensure it receives the necessary priority. Proper signatures and information from the provider are crucial.
This form is specifically for outpatient services. Inpatient services require different procedures and forms.
While processing times are specified, you may receive updates or requests for additional information during the review process. Stay proactive in checking the status.
Filling out the Ambetter Outpatient Authorization Form correctly is crucial for ensuring timely approval of healthcare services. Here are four key takeaways to keep in mind: