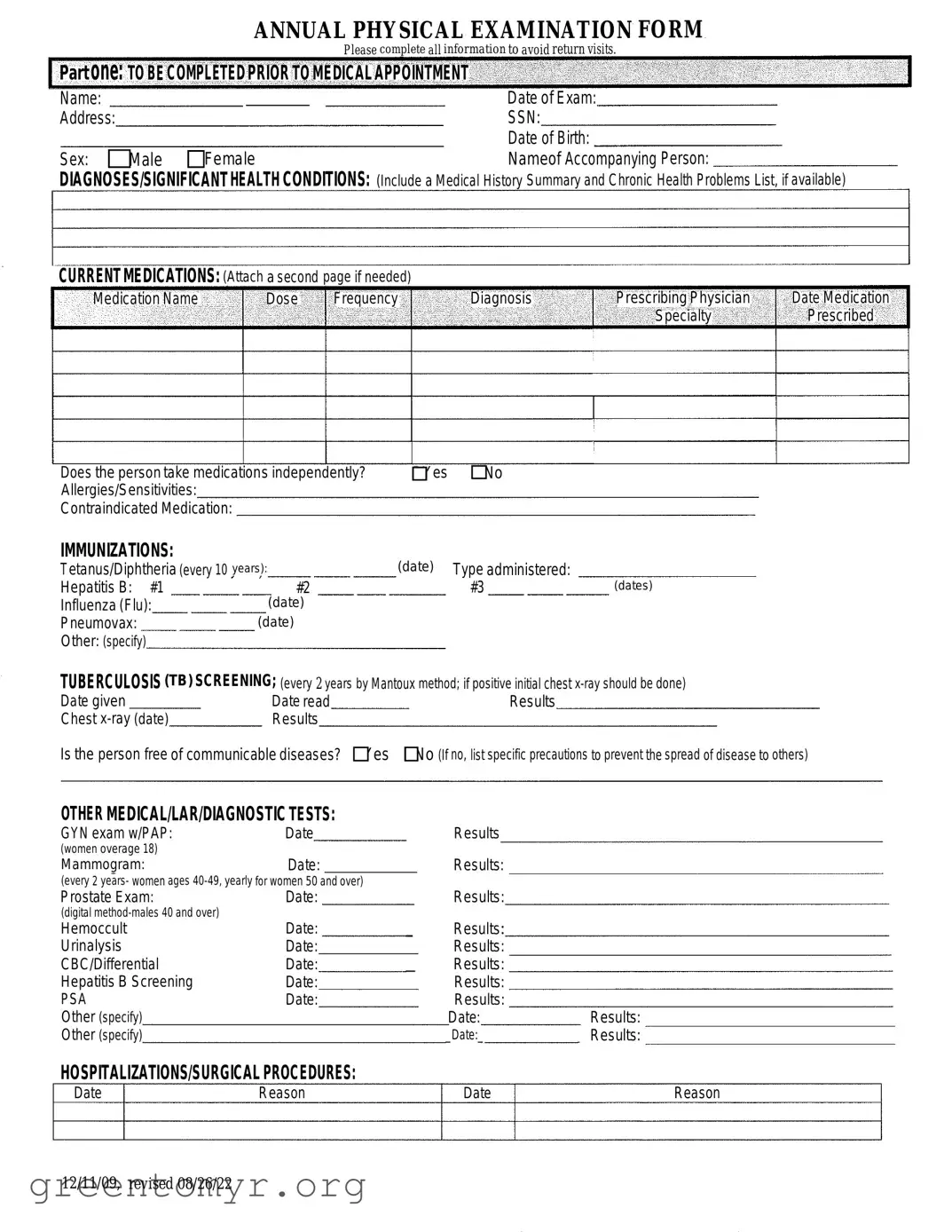
The Annual Physical Examination form is a vital tool that helps healthcare providers gather comprehensive information about a patient’s health before their medical appointment. This form includes essential sections that require patients to provide personal details such as their name, date of birth, and address, as well as significant medical history and current medications. It prompts patients to disclose any allergies or sensitivities and lists required immunizations, ensuring that healthcare providers have a complete picture of the patient's vaccination status. Additionally, the form covers various medical tests and screenings, such as tuberculosis screening and cancer screenings, tailored to different age groups and genders. Patients are also asked to report any hospitalizations or surgical procedures they have undergone, which can be crucial for understanding their health background. The second part of the form focuses on the general physical examination, where vital signs like blood pressure and pulse are recorded, alongside evaluations of different body systems. By completing this form accurately, patients can help streamline their visit, allowing healthcare professionals to provide better care based on informed assessments.
|
ANNUAL PHYSICAL EXAMINATION FORM |
|
|
|
Please complete all information to avoid return visits. |
Part one: TOBE COMPLETEDPRIOR TOMEDICAL APPOINTMENT |
||
Name: |
— |
Date of Exam: |
Address: |
|
SSN: |
|
|
Date of Birth: |
Sex: OMale |
DFemale |
Nameof Accompanying Person: |
DIAGNOSES/SIGNIFICANTHEALTH CONDITIONS: (Include a Medical History Summary and Chronic Health Problems List, if available)
CURRENTMEDICATIONS: (Attach a second page if needed)
Medication Name |
Dose |
Frequency |
Diagnosis |
Prescribing Physician |
Date Medication |
|
|
|
|
Specialty |
Prescribed |
Does the person take medications independently? |
DYes |
DNo |
Allergies/Sensitivities: |
|
|
Contraindicated Medication: |
|
|
IMMUNIZATIONS:
Tetanus/Diphtheria (every 10 years): |
(date) Type administered: |
|
|
Hepatitis B: #1 |
#2 |
#3 |
(dates) |
Influenza (Flu): |
(date) |
|
|
Pneumovax: |
(date) |
|
|
Other: (specify)
TUBERCULOSIS (TB) SCREENING; (every 2 years by Mantoux method; if positive initial chest
Date given |
Date read |
Results |
Chest |
Results |
|
Is the person free of communicable diseases? DYes |
DNo (If no, list specific precautions to prevent the spread of disease to others) |
|
OTHER MEDICAL/LAR/DIAGNOSTIC TESTS:
GYN exam w/PAP: |
Date |
Results |
(women overage 18)
Mammogram:Date:
(every 2 years- women ages
Prostate Exam: |
Date: |
(digital |
Date: |
Hemoccult |
|
Urinalysis |
Date: |
CBC/Differential |
Date: |
Hepatitis B Screening |
Date: |
PSA |
Date: |
Other (specify) |
|
Other (specify) |
|
|
Results: |
|
_ |
Results: |
|
Results: |
|
|
_ |
Results: |
|
Results: |
|
|
|
Results: |
|
|
Results: |
|
|
Date: |
Results: |
|
_Date:_ |
_ Results: |
HOSPITALIZATIONS/SURGICALPROCEDURES:
Date |
Reason |
Date |
Reason |
12/11/09, revised 08/26/22
Name: |
|
|
|
Date of Exam: |
|
|
Part TWO: GENERALPHYSICALEXAMINATION |
|
|
|
|
||
|
|
Please complete all information to avoid return visits. |
|
|
||
Blood Pressure: |
/ |
Pulse: |
Respirations: |
Temp: |
Height: |
Weight: |
EVALUATIONOFSYSTEMS |
|
Comments/Description |
||||
System Name |
|
Normal Findings? |
|
|||
Eyes |
|
|
|
|
|
|
Ears |
|
|
|
|
|
|
Nose |
|
|
|
|
|
|
Mouth/Throat |
|
|
|
|
|
|
Head/Face/Neck |
|
|
|
|
|
|
Breasts |
|
|
|
|
|
|
Lungs |
|
|
|
|
|
|
Cardiovascular |
|
|
|
|
|
|
Extremities |
|
|
|
|
|
|
Abdomen |
|
|
|
|
|
|
Gastrointestinal |
|
|
|
|
|
|
Musculoskeletal |
|
|
|
|
|
|
Integumentary |
|
|
|
|
|
|
Renal/Urinary |
|
|
|
|
|
|
Reproductive |
|
|
|
|
|
|
Lymphatic |
|
|
|
|
|
|
Endocrine |
|
|
|
|
|
|
Nervous System |
|
|
Is further evaluation recommended by specialist? |
DYes |
||
VISION SCREENING |
|
|
||||
HEARING SCREENING |
|
|
Is further evaluation recommended by specialist? |
DYes |
||
Additional Comments: |
|
|
|
|
|
|
Medical history summary reviewed? DYes |
DNo |
|
|
|
||
Medication added, changed, or deleted: (from this appointment)
Special medication considerations or side effects:
Recommendations for health maintenance: (include need for lab work at regular intervals, treatments, therapies, exercise, hygiene, weight control, etc.)
Recommendations for manual breast exam or manual testicular exam: (include who will perform and frequency)
Recommended diet and special instructions:
Information pertinent to diagnosis and treatment in case of emergency:
Limitations or restrictions for activities (including work day, lifting, standing, and bending): |
DNo |
DYes (specify) |
||
Does this person use adaptive equipment? |
DNo |
DYes (specify): |
|
|
Change in health status from previous year? DNo |
DYes (specify): |
|
|
|
This individual is recommended for ICF/ID level of care? (see attached explanation) |
DYes |
DNo |
||
Specialty consults recommended? DNo |
QYes (specify): |
|
|
|
Seizure Disorder present? DNo OYes (specify type): |
|
|
Date of Last Seizure: |
|
Name of Physician (please print) |
Physician’s Signature |
|
Date |
|
Physician Address: |
|
Physician Phone Number: |
||
Created 12/11/09, revised 08/14/2023
| Fact Name | Description |
|---|---|
| Purpose of the Form | The Annual Physical Examination Form is designed to gather essential health information before a medical appointment. |
| Patient Information | It requires personal details such as name, date of birth, address, and social security number to ensure accurate identification. |
| Medical History | Patients must disclose any significant health conditions and current medications, including allergies and sensitivities. |
| Immunization Records | The form includes a section for documenting immunizations, ensuring that vaccinations are up to date. |
| Screening Tests | It lists various recommended screenings, such as TB tests and cancer screenings, to promote preventive care. |
| State-Specific Regulations | In some states, specific laws govern the use and requirements of this form, ensuring compliance with health regulations. |
| Follow-Up Recommendations | After the examination, the form provides space for health maintenance recommendations and any necessary follow-up actions. |
Completing the Annual Physical Examination form accurately is crucial for a smooth medical appointment. After filling out the form, you will submit it to your healthcare provider, who will use the information to assess your health status and provide appropriate care.
To fill out the Annual Physical Examination form, you need to provide several key details. Start with your name, date of exam, address, Social Security Number, date of birth, and sex. If someone is accompanying you, include their name as well. You should also list any significant health conditions or diagnoses, current medications, allergies, and immunization history. If you have had any recent medical tests or procedures, include those results too. Completing all sections helps ensure a smooth appointment and avoids the need for follow-up visits.
The Annual Physical Examination form should be completed once a year, prior to your medical appointment. This yearly update helps your healthcare provider stay informed about your health status, any changes in medications, and recent medical history. If you experience any significant health changes or start new medications outside of your annual exam, it’s a good idea to update your form sooner.
If you have a medical condition or take multiple medications, be sure to provide detailed information on the form. List each medication, its dosage, frequency, and the diagnosis it treats. If you have allergies or sensitivities to certain medications, include that information as well. If necessary, attach an additional page for more details. This information is crucial for your healthcare provider to make informed decisions about your care.
If you forget to fill out part of the Annual Physical Examination form, it may lead to delays during your appointment. Incomplete forms can require follow-up visits to gather missing information. To avoid this, double-check your form before your appointment. If you realize you've missed something after submitting it, contact your healthcare provider's office as soon as possible to correct the information.
Filling out the Annual Physical Examination form accurately is crucial for ensuring a smooth medical appointment. However, many individuals make common mistakes that can lead to complications or delays in their care. One frequent error is leaving sections incomplete. For example, failing to provide basic information such as the date of birth or current medications can result in the need for a follow-up visit. It’s essential to fill out every section to avoid unnecessary delays.
Another mistake involves not updating medical history or current medications. Many people forget to include recent changes in their health status or new medications they have started. This oversight can lead to potential health risks during the examination. Keeping the information current helps healthcare providers make informed decisions about your care.
Additionally, some individuals may not fully disclose allergies or sensitivities. This information is vital for preventing adverse reactions during treatment. If a person has experienced allergic reactions to medications or other substances, it’s important to list these clearly on the form. Omitting this information can compromise safety during the examination process.
Lastly, misunderstanding the requirements for immunizations is a common issue. Many people do not realize that specific vaccines need to be documented with exact dates. For instance, the Tetanus/Diphtheria shot must be updated every ten years, and missing this detail can lead to complications. Accurately recording immunization history ensures that healthcare providers have a complete picture of your health status.
The Annual Physical Examination form is an essential document that helps healthcare providers assess a patient's overall health. However, several other forms and documents often accompany this examination. Each of these documents serves a unique purpose in ensuring comprehensive care and accurate health records.
Each of these forms plays a vital role in the healthcare process. Together, they help ensure that patients receive thorough and personalized care, while also protecting their rights and privacy.
The Annual Physical Examination form serves a vital role in healthcare, ensuring that patients receive comprehensive evaluations. It shares similarities with several other important documents in the medical field. Here are four documents that are akin to the Annual Physical Examination form:
When filling out the Annual Physical Examination form, it's important to ensure accuracy and completeness. Here’s a list of things you should and shouldn't do to make the process smoother.
By following these guidelines, you can help facilitate a more efficient and effective examination process. Your attention to detail is key to receiving the best care possible.
Misconceptions about the Annual Physical Examination form can lead to confusion and missed opportunities for important health care. Here are five common misunderstandings:
Completing the Annual Physical Examination form accurately is essential for ensuring a smooth medical appointment. Here are some key takeaways to consider: