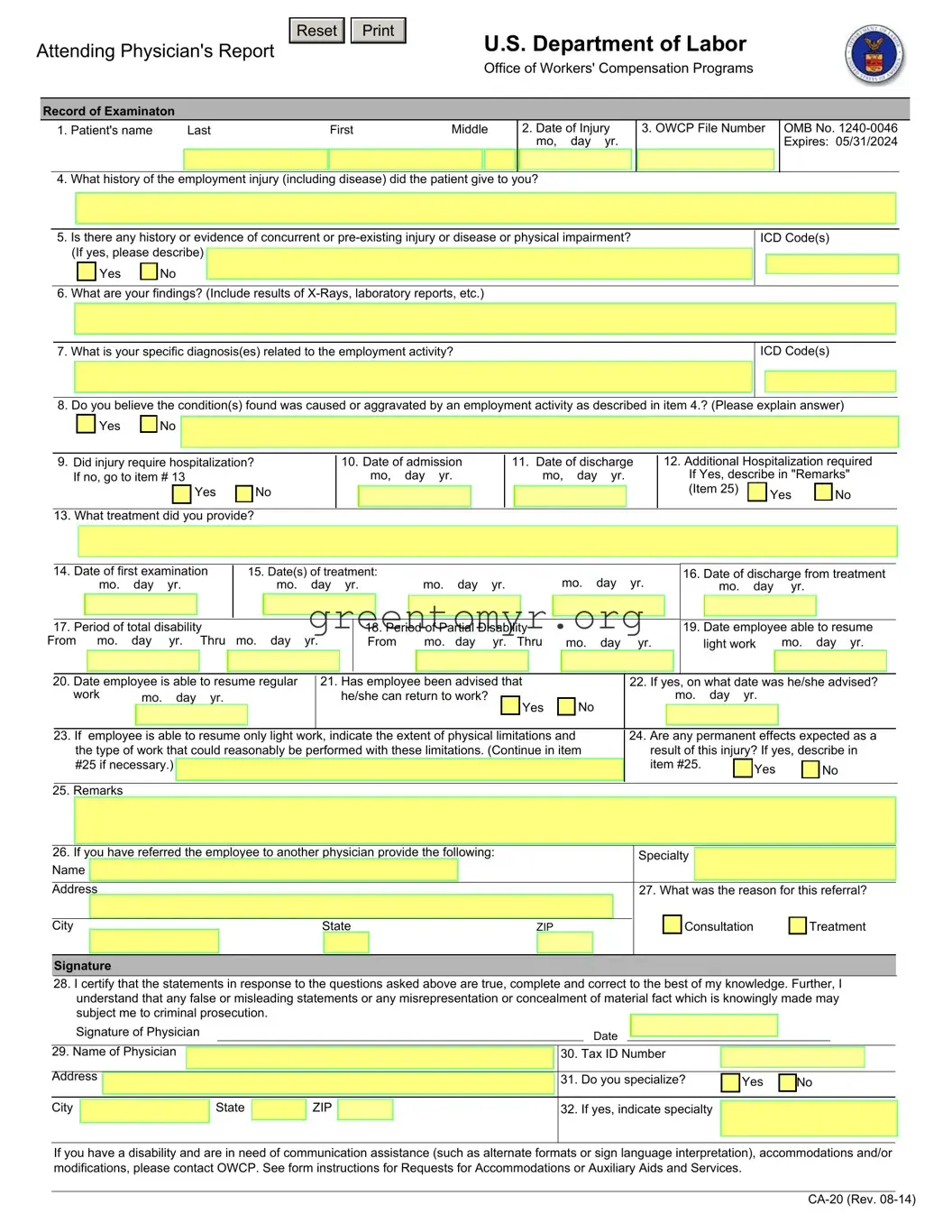
The CA-20 form, known as the Attending Physician's Report, plays a crucial role in the workers' compensation process within the United States. This document is essential for documenting the medical condition of an employee who has sustained a work-related injury or illness. Designed to gather comprehensive information, the CA-20 includes key sections that require the physician to record the patient's personal details, the date of the injury, and the patient's account of how the injury occurred. Furthermore, the form prompts physicians to assess the history of any concurrent or pre-existing conditions and to provide detailed medical findings, including diagnoses and treatment plans. It also inquiries into the degree of disability—both total and partial—and whether the employee can return to regular or light work. The form must be completed thoroughly, as it serves as a critical piece of evidence in the compensation claim process. Ensuring its accuracy and completeness is vital, as the information collected directly impacts the determination of benefits for the injured worker.
Attending Physician's Report
Reset 

U.S. Department of Labor
Office of Workers' Compensation Programs
Record of Examinaton
1. Patient's name |
Last |
First |
Middle |
|
2. Date of Injury |
||
|
|
|
|
|
|
|
mo, day yr. |
|
|
|
|
|
|
|
|
4. What history of the employment injury (including disease) did the patient give to you?
3. OWCP File Number
OMB No.
5.Is there any history or evidence of concurrent or
Yes |
|
No |
6. What are your findings? (Include results of
ICD Code(s)
7. What is your specific diagnosis(es) related to the employment activity?
ICD Code(s)
8. Do you believe the condition(s) found was caused or aggravated by an employment activity as described in item 4.? (Please explain answer)
Yes |
|
No |
9.Did injury require hospitalization? If no, go to item # 13
Yes |
|
No |
|
13. What treatment did you provide?
10.Date of admission mo, day yr.
11.Date of discharge mo, day yr.
12.Additional Hospitalization required If Yes, describe in "Remarks"
(Item 25) |
Yes |
No |
|
|
|
14. Date of first examination |
|
15. Date(s) of treatment: |
|
mo. |
day |
yr. |
|
mo. |
day |
yr. |
|
|
|
16. Date of discharge from treatment |
||||||||||||||||||||||||||||||||||
|
|
|
|
mo. |
day |
yr. |
|
|
|
|
mo. |
day |
yr. |
|
|
|
|
|
|
|
mo. |
|
day |
|
yr. |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17. Period of total disability |
|
|
|
|
|
|
|
18. Period of Partial Disability |
|
|
|
|
|
|
|
|
|
|
|
19. Date employee able to resume |
||||||||||||||||||||||||||||
From |
mo. |
day |
yr. |
Thru |
mo. day |
yr. |
|
From |
|
mo. |
day |
yr. Thru |
|
mo. |
day |
|
yr. |
|
light work |
mo. day yr. |
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
20. Date employee is able to resume regular |
|
21. Has employee been advised that |
|
|
|
|
|
|
22. If yes, on what date was he/she advised? |
|||||||||||||||||||||||||||||||||||||||
|
|
work |
|
mo. |
|
day |
yr. |
|
|
|
|
|
|
he/she can return to work? |
|
|
Yes |
|
|
No |
|
|
|
|
|
|
mo. |
day |
yr. |
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
23. If |
employee is able to resume only light work, indicate the extent of physical limitations and |
|
|
24. Are any permanent effects expected as a |
||||||||||||||||||||||||||||||||||||||||||||
|
|
|
the type of work that could reasonably be performed with these limitations. (Continue in item |
|
|
|
|
result of this injury? If yes, describe in |
||||||||||||||||||||||||||||||||||||||||||
|
|
|
#25 if necessary.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
item #25. |
|
|
|
Yes |
|
|
|
No |
|||||||||
|
|
25. Remarks |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
26. If you have referred the employee to another physician provide the following: |
|
|
|
|
|
|
|
Specialty |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
27. What was the reason for this referral? |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Consultation |
|
|
Treatment |
|||||||||
|
City |
|
|
|
|
|
|
|
|
|
|
|
State |
|
|
|
|
|
|
ZIP |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature
28.I certify that the statements in response to the questions asked above are true, complete and correct to the best of my knowledge. Further, I understand that any false or misleading statements or any misrepresentation or concealment of material fact which is knowingly made may subject me to criminal prosecution.
Signature of Physician |
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
29. Name of Physician |
|
|
|
|
|
|
|
30. |
Tax ID Number |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Address |
|
|
|
|
|
|
|
|
31. |
Do you specialize? |
|
Yes |
|
No |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
State |
|
ZIP |
|
|
|
32. |
If yes, indicate specialty |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If you have a disability and are in need of communication assistance (such as alternate formats or sign language interpretation), accommodations and/or modifications, please contact OWCP. See form instructions for Requests for Accommodations or Auxiliary Aids and Services.
INSTRUCTIONS TO PHYSICIAN FOR COMPLETING ATTENDING PHYSICIAN'S REPORT
1.COMPLETE THE ENTRIES
2.IF DISABILITY HAS NOT TERMINATED, INDICATE IN ITEM 17; AND
3.SEND THE FORM AND YOUR BILL TO:
Office of Workers’ Compensation Programs
Division of Federal Employees’, Longshore and Harbor Workers’ Compensation
Federal Employees’ Compensation Act
PO Box 8311
London, KY
IMPORTANT: A medical report is required by the Office of Workers' Compensation Programs before payment of compensation for loss of wages or permanent disability can be made to the employee.
This information is required to obtain or retain a benefit (5 U.S.C. 8101, et seq.). If you have submitted a narrative medical report or a form
OWCP requires that medical bills, other than hospital bills, be submitted on the American Medical Association health insurance claim form, HCFA
INSTRUCTIONS FOR THE INJURED WORKER/ EMPLOYING AGENCY
Compensation for wage loss cannot be paid unless medical evidence has been submitted supporting disability for work during the period claimed. For claims based on traumatic injury and reported on Form
For payment of a schedule award the claimant must have a permanent loss or loss of function of one of the members of the body or organs enumerated in the regulations (20 C.F.R. 10.404). The attending physician must affirm that maximum medical improvement of the condition has been reached and should describe the functional loss and the resulting impairment in accordance with the American Association Guides to the Evaluation of Permanent Impairment.
Notice
Requests for Accommodations or Auxiliary Aids and Services
If you have a disability, federal law gives you the right to receive help from the OWCP in the form of communication assistance, accommodation(s) and/or modification(s) to aid you in the claims process. For example, we will provide you with copies of documents in alternate formats, communication services such as sign language interpretation, or other kinds of adjustments or changes to accommodate your disability. Please contact our office or your OWCP claims examiner to ask about this assistance.
Privacy Act Statement
In accordance with the Privacy Act of 1974, as amended (5 U.S.C. 552a), you are here by notified that: (1) The Federal Employees' Compensation Act, as amended and extended (5 U.S.C. 8101, et seq.) (FECA) is administered by the Office of Workers' Compensation Programs of the U. S .Department of Labor, which receives and maintains personal information on claimants and their immediate families. (2) Information which the Office has will be used to determine eligibility for and the amount of benefits payable under the FECA, and may be verified through computer matches or other appropriate means. (3) Information may be given to the Federal agency which employed the claimant at the time of injury in order to verify statements made, answer questions concerning the status of the claim, verify billing, and to consider issues relating to retention, rehire, or other relevant matters. (4) Information may also be given to other Federal agencies, other government entities, and to
Public Burden Statement
According to the Paperwork Reduction Act of 1995, no persons are required to respond to this collection of information unless it displays a currently valid OMB control number. Public reporting burden for this collection of information is estimated to average 5 minutes per response, including time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. The obligation to respond to this collection is required to obtain or retain a benefit under 5 U.S.C. 8101, et seq. Send comments regarding the burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to the U.S. Department of Labor, Office of Workers' Compensation Programs, Room
| Fact Name | Description |
|---|---|
| Purpose | The CA-20 form is used to document an attending physician's report related to a patient's employment-related injury. |
| Governing Law | The CA-20 form is governed by the Federal Employees' Compensation Act (FECA), 5 U.S.C. 8101, et seq. |
| Submission Process | Physicians must complete the form in full and submit it along with their bill to the Office of Workers’ Compensation Programs. |
| Hospitalization | The form includes sections to cover hospitalization details and treatment provided, ensuring comprehensive reporting. |
| Privacy Regulations | The Privacy Act of 1974 mandates how personal information is handled, ensuring confidentiality in the claims process. |
Filling out the CA-20 form is essential for capturing necessary medical details related to a worker's injury. Accurate completion ensures the timely processing of claims for compensation. Below are the steps required to fill out this important form.
Once completed, ensure that it is sent to the appropriate office along with any necessary documentation to support the injury claim effectively.
The CA-20 form is used to report the attending physician's medical findings and opinions regarding an injured worker's condition. It is crucial for processing claims under the Office of Workers' Compensation Programs (OWCP). The information gathered helps determine eligibility for wage loss and disability benefits. Accurate and complete submissions can expedite the claims process.
The CA-20 form must be completed by the attending physician who treated the injured employee. This includes specialists who may have provided evaluation or treatment related to the injury. It is important that the physician provides detailed and accurate information regarding the injury, its effects, and any necessary treatments.
The form requires a variety of information, including:
Completing all sections thoroughly is crucial for a successful claim.
The CA-20 form is integral to the compensation process. It provides the necessary medical evidence to support a claim for wage loss or disability benefits. Without this information, employees cannot receive compensation for their time off work. The form must be sent to OWCP by the physician directly.
If the form is incomplete or contains inaccuracies, it may lead to delays in processing the claim. In some cases, it could result in a denial of benefits. To avoid these issues, it is essential for the attending physician to review all information thoroughly before submission.
No, the CA-20 form must be completed and submitted by the attending physician. However, the employee is responsible for ensuring the physician receives the necessary information and submits the form promptly. Clear communication between the employee and the physician can help minimize delays.
The remarks section should provide any additional relevant information that does not fit in the standard questions. This can include further explanations of diagnoses, the specifics of treatment plans, and any particulars about the employee’s ability to return to work. Detailed notes can assist in clarifying the case.
Yes, assistance is available for individuals who may have disabilities affecting their ability to complete the CA-20 form. The OWCP offers communication assistance and can provide forms in alternate formats. It is important to contact the OWCP office for specific accommodations that may be necessary.
When completing the CA-20 form, individuals often encounter pitfalls that can lead to delays or issues with their claims. One common mistake is failing to provide complete and accurate patient information. Missing details such as the patient’s full name, date of injury, or OWCP file number can create significant problems in processing the claim. Each field must be filled out precisely to ensure the information is captured correctly.
Another frequent error is not thoroughly documenting the history of the employment injury. Item 4 requires a clear account of what the patient reported regarding their injury. Inadequate or vague descriptions may hinder the claim's assessment. The physician should ensure that this section is detailed and specific, covering all aspects the patient described.
The form’s section on pre-existing conditions often sees oversight as well. In item 5, if there is any history or evidence of prior injuries or ailments, it is crucial to disclose this information. Omitting such details can lead to complications or misunderstandings when evaluating the claim.
Many individuals also struggle with providing insufficient findings and diagnoses. In item 6 and item 7, comprehensive notes on physical findings, test results, and specific diagnoses are essential. Neglecting to include this information can result in a lack of supporting medical evidence, which is key to justifying the claim.
Additionally, answering the questions regarding causation and ability to return to work may be overlooked. Specifically, item 8 focuses on whether employment activities caused or aggravated the condition. A clear explanation is needed here, as it directly impacts the outcome of the claim. Similarly, determination about the return to work should be backed by factual medical evaluations, addressing expectations and limitations thoroughly.
Finally, signing the form without reviewing all entries can lead to critical mistakes. It's essential that the physician double-checks all information for accuracy before submitting the form. Mistakes or corrections made after submission can cause delays for the patient and complicate the claims process significantly.
The CA-20 form, known as the Attending Physician's Report, is an essential document in the process of claiming workers' compensation benefits in the United States. It provides valuable insights from a medical professional regarding the nature of an injury, its impact on the employee's ability to work, and the necessary treatments. Alongside the CA-20 form, several other documents are often required to ensure a complete and accurate claim. Below is a brief overview of these accompanying forms and documents.
Understanding these forms is crucial for navigating the workers' compensation system effectively. Each document plays a pivotal role in establishing your case, ensuring that the necessary medical evidence and details are communicated clearly to support the claim. Ensuring all paperwork is properly completed and promptly submitted can significantly impact the timeliness of obtaining benefits.
When filling out the CA-20 form, follow these guidelines to ensure correctness and compliance.
Understanding the CA-20 form can be challenging. Many misunderstand its purpose and requirements. Here are four common misconceptions:
Being aware of these misconceptions can help ensure that the correct information is provided, improving the chances of a successful claim.
Key Takeaways for Filling Out and Using the CA-20 Form