When it comes to ensuring the well-being of residents in care facilities, the CNA Shower Sheets form serves as an essential tool for Certified Nursing Assistants (CNAs). This form not only facilitates a thorough visual assessment of a resident's skin during shower time but also provides a structured way to document any abnormalities. CNAs are responsible for identifying issues such as bruising, skin tears, rashes, and more, which can significantly impact a resident's health. By using the body chart included in the form, CNAs can pinpoint and describe these abnormalities accurately, ensuring that any concerns are communicated effectively to the charge nurse and ultimately to the Director of Nursing (DON). Additionally, the form includes a section to determine if the resident requires toenail care, highlighting the comprehensive nature of skin monitoring. The signatures from both the CNA and charge nurse confirm that the assessment has been completed and reviewed, creating a clear chain of responsibility. With this structured approach, the CNA Shower Sheets form plays a vital role in maintaining skin integrity and promoting the overall health of residents.
Skin Monitoring: Comprehensive CNA Shower Review
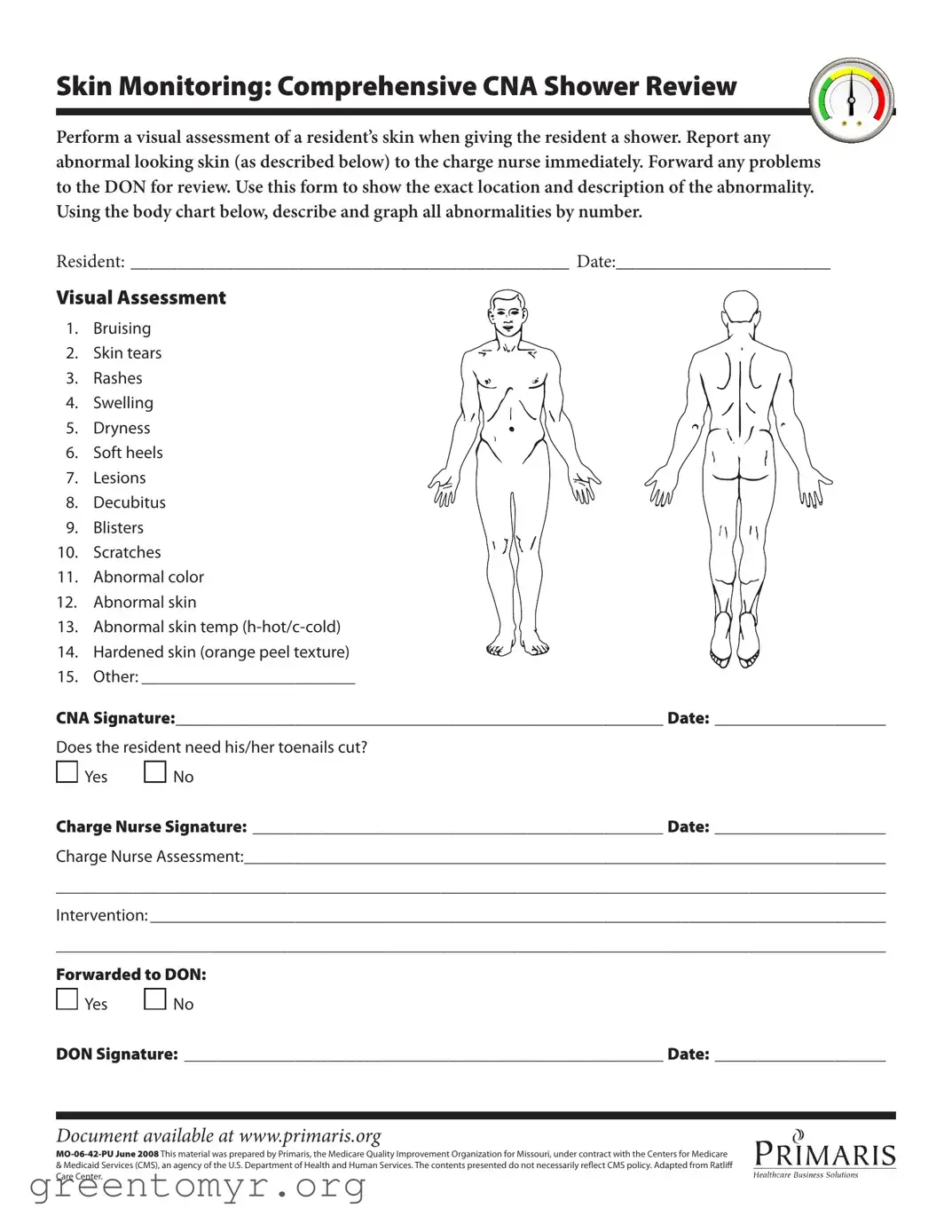
Perform a visual assessment of a resident’s skin when giving the resident a shower. Report any abnormal looking skin (as described below) to the charge nurse immediately. Forward any problems to the DON for review. Use this form to show the exact location and description of the abnormality. Using the body chart below, describe and graph all abnormalities by number.
RESIDENT: _______________________________________________ DATE:_______________________
Visual Assessment
1. Bruising
2. Skin tears
3. Rashes
4. Swelling
5. Dryness
6. Soft heels
7. Lesions
8. Decubitus
9. Blisters
10. Scratches
11. Abnormal color
12. Abnormal skin
13. Abnormal skin temp
14. Hardened skin (orange peel texture)
15. Other: _________________________
CNA Signature:_________________________________________________________ Date: ____________________
Does the resident need his/her toenails cut?
Yes No
Charge Nurse Signature: ________________________________________________ Date: ____________________
Charge Nurse Assessment:___________________________________________________________________________
_________________________________________________________________________________________________
Intervention: ______________________________________________________________________________________
_________________________________________________________________________________________________
Forwarded to DON:
Yes No
DON Signature: ________________________________________________________ Date: ____________________
Document available at www.primaris.org
&Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily relect CMS policy. Adapted from Ratlif Care Center.
| Fact Name | Details |
|---|---|
| Purpose | The CNA Shower Sheets form is used for documenting skin assessments during resident showers. |
| Skin Monitoring | CNA staff must perform a visual assessment of the resident's skin and report any abnormalities. |
| Types of Abnormalities | Common abnormalities include bruising, skin tears, rashes, swelling, and lesions. |
| Documentation | Staff must describe and graph abnormalities on a body chart included in the form. |
| Signatures Required | The form requires signatures from the CNA, charge nurse, and Director of Nursing (DON). |
| State-Specific Law | In Missouri, the governing law includes regulations from the Missouri Department of Health and Senior Services. |
| Additional Notes | The document also includes a section for assessing the need for toenail care. |
Filling out the CNA Shower Sheets form is an important task that helps ensure residents receive proper skin assessments during showers. Following these steps will guide you through the process of completing the form accurately.
The CNA Shower Sheets form serves as a tool for Certified Nursing Assistants (CNAs) to document skin assessments during resident showers. It allows CNAs to visually assess and report any abnormalities in a resident's skin, such as bruising, rashes, or lesions. This documentation is crucial for ensuring that any issues are communicated to the charge nurse and the Director of Nursing (DON) for further evaluation and intervention.
When filling out the visual assessment section, CNAs should carefully examine the resident's skin during the shower. If any abnormalities are observed, they should be noted in the appropriate categories listed on the form. For each abnormality, use the body chart provided to indicate the exact location and describe the issue by number. This helps in tracking changes over time and ensures accurate communication with the nursing staff.
If you notice an abnormality during the skin assessment, it is essential to report it to the charge nurse immediately. This ensures that the issue is addressed promptly. After reporting, the problem should be forwarded to the DON for review. Proper documentation using the form is critical, as it provides a record of the findings and actions taken.
Yes, the CNA Shower Sheets form includes a section that asks whether the resident needs their toenails cut. CNAs should assess the condition of the resident's toenails and mark "Yes" or "No" accordingly. If toenail care is needed, it should be addressed as part of the overall skin and personal care during the shower.
Filling out the CNA Shower Sheets form requires attention to detail. One common mistake is failing to accurately document the resident's name and date at the top of the form. Omitting this information can lead to confusion and miscommunication regarding the resident's care.
Another frequent error involves incomplete visual assessments. CNAs may skip certain areas of the body or fail to check for all listed abnormalities. It is essential to perform a thorough examination and report any issues, as incomplete assessments can result in undetected skin problems.
Misidentifying or mislabeling skin conditions is also a prevalent issue. For instance, a rash may be mistaken for a bruise, or a skin tear may not be documented correctly. Accurate descriptions are crucial for effective communication with the charge nurse and for appropriate interventions.
CNAs sometimes forget to use the body chart provided in the form. This chart is necessary for graphing the exact locations of any abnormalities. Neglecting to utilize this tool can hinder the clarity of the report and complicate follow-up actions.
Another mistake occurs when CNAs do not sign and date the form after completing their assessments. This signature is vital for accountability and ensures that the information is officially recorded. Without it, there may be questions about the validity of the reported findings.
Failing to indicate whether the resident needs toenail care is another oversight. This section is important for maintaining the resident's overall hygiene and comfort. Leaving it blank can lead to missed opportunities for necessary care.
In some cases, CNAs may forget to forward the completed form to the Director of Nursing (DON). This step is critical for ensuring that any identified issues receive appropriate attention and follow-up. Not forwarding the form can delay necessary interventions.
Lastly, CNAs may neglect to document the charge nurse's assessment and any interventions taken. This information is essential for continuity of care and helps ensure that all team members are informed about the resident's condition and treatment plan.
The CNA Shower Sheets form plays a crucial role in documenting skin assessments during resident showers. Alongside this form, several other documents are commonly used to ensure comprehensive care and accurate record-keeping. Below is a list of these documents, each serving a specific purpose in the care process.
These documents, when used in conjunction with the CNA Shower Sheets form, contribute to a holistic approach to resident care. They ensure that all aspects of a resident's health and well-being are monitored and addressed effectively.
The CNA Shower Sheets form is an important tool for monitoring residents' skin health during showering. It shares similarities with several other documents used in healthcare settings. Here are eight documents that are similar to the CNA Shower Sheets form, along with a brief explanation of how they relate:
Each of these documents plays a crucial role in ensuring comprehensive care and monitoring of residents, just like the CNA Shower Sheets form. Together, they help create a holistic approach to patient health and safety.
When filling out the CNA Shower Sheets form, it's essential to approach the task with care and attention to detail. Here’s a list of what to do and what to avoid to ensure accurate and effective documentation.
By following these guidelines, you can ensure that the CNA Shower Sheets form is completed accurately, helping to maintain the highest standards of care for residents.
Here are some common misconceptions about the CNA Shower Sheets form:
When utilizing the CNA Shower Sheets form, there are several important aspects to keep in mind. Understanding these key points can enhance the effectiveness of skin monitoring during resident care.
By adhering to these guidelines, caregivers can ensure that residents receive the best possible care and that any skin issues are promptly addressed.