The Dap Note Sample form is an essential tool in both clinical practice and documentation for therapists. This structured format allows mental health professionals to capture pertinent information regarding client sessions effectively. The form is divided into three primary components: "D," "A," and "P." "D" encompasses both subjective and objective data about the client, highlighting what the client shares or feels alongside observable behaviors noted by the therapist. For instance, statements like "Depression appears improved this week" offer a glimpse into the client’s progress. The "A" section provides insight into the intervention strategies employed and the assessment of the client's current status, helping therapists formulate working hypotheses. Finally, the "P" part outlines the therapist's plans moving forward, including scheduling future sessions and addressing specific topics for discussion or homework assignments. By following this framework, therapists can maintain clear and effective case notes that serve not only as a valuable resource for treatment planning but also contribute to continuity of care in multidisciplinary settings.
CASE NOTE FORMAT - DAP CHARTING
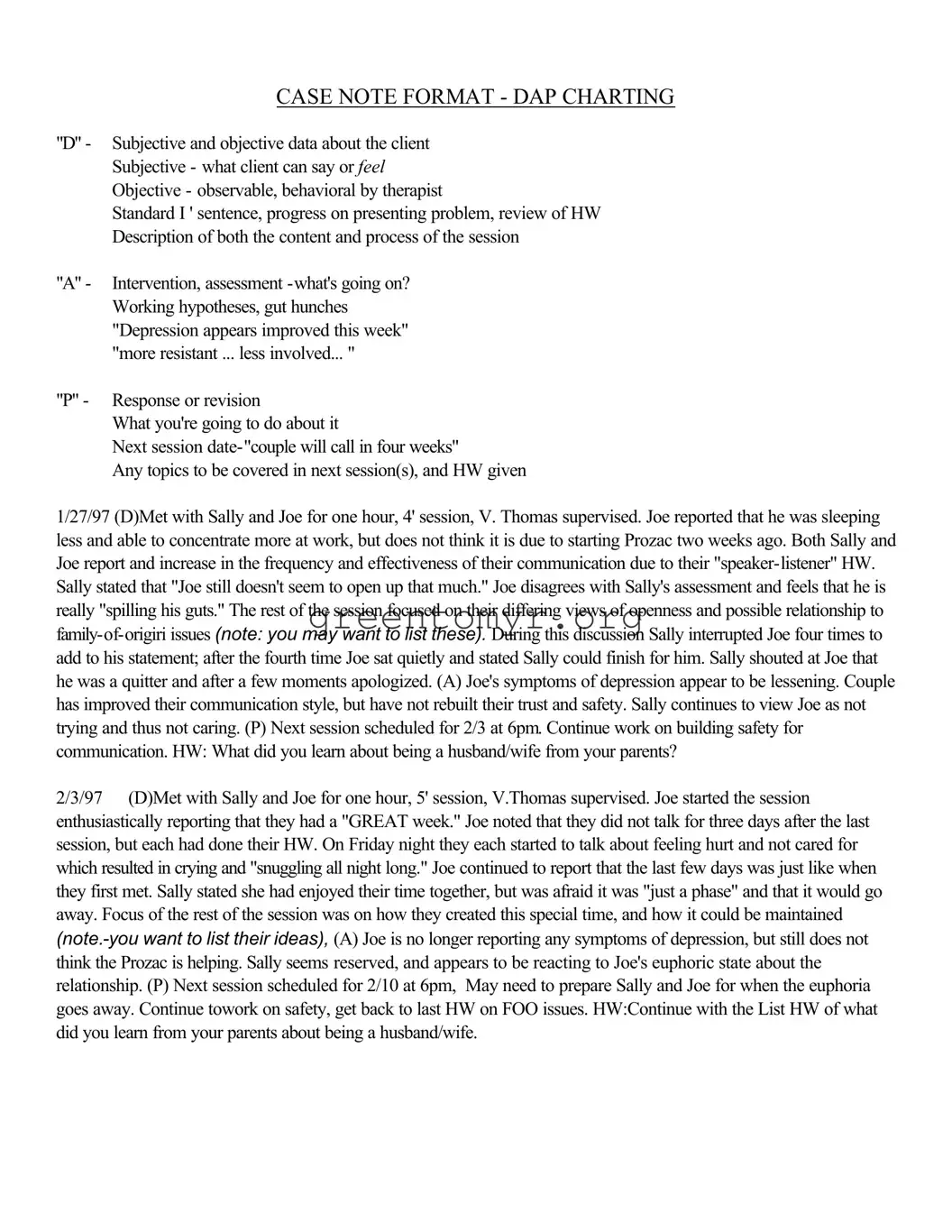
"D" - Subjective and objective data about the client Subjective - what client can say or FEEL Objective - observable, behavioral by therapist
Standard I ' sentence, progress on presenting problem, review of HW Description of both the content and process of the session
"A" - Intervention, assessment
"P" - Response or revision
What you're going to do about it
Next session
Any topics to be covered in next session(s), and HW given
1/27/97 (D)Met with Sally and Joe for one hour, 4' session, V. Thomas supervised. Joe reported that he was sleeping less and able to concentrate more at work, but does not think it is due to starting Prozac two weeks ago. Both Sally and Joe report and increase in the frequency and effectiveness of their communication due to their
2/3/97 (D)Met with Sally and Joe for one hour, 5' session, V.Thomas supervised. Joe started the session enthusiastically reporting that they had a "GREAT week." Joe noted that they did not talk for three days after the last session, but each had done their HW. On Friday night they each started to talk about feeling hurt and not cared for which resulted in crying and "snuggling all night long." Joe continued to report that the last few days was just like when they first met. Sally stated she had enjoyed their time together, but was afraid it was "just a phase" and that it would go away. Focus of the rest of the session was on how they created this special time, and how it could be maintained
|
Writing Behavioral Goals |
Lends itself to any 2 people agreeing the goal is met |
|
Subject + verb |
|
Action |
|
Frequency |
|
Duration |
|
Monitor |
|
Goals:
·Measurable
·Observable
·
·
·Realistic (achievable)
·Relevant (to the problem)
·Appropriate
·Consistent with the client's values
·Should be able to describe what the client should be able to do to demonstrate improvement/symptom relief
Everything You Ever Wanted To Know About Case Notes
·Think about what you are going to write and formulate before you begin
·Be sure you have the right chart!
·Date and sign every entry
·Proofread
·Record as "late entry" anytime it doesn't fall in chronological order; be timely
·Think about how the client comes through on paper
·Watch
·Errors should have a line through incorrect information. Write error,intital and date
·Write neatly and legibly; print if handwriting is difficult to read
·Use proper spelling, grammar and sentence structure
·Don't leave blank spaces between entries; can imply vital information left out
·Put client name/case number on each page
·Avoid slang,curse words
·Another provider should be able to continue quality care
·Use quotes from client that are clinically pertinent Use descriptive terms
·Describe what you observed, not just your opinion of what you observed
·Reference identified problems from the treatment plan
·Reference diagnostic criteria from
·Use power quotes:
"Client remains at risk for _____________ as evidenced by ___________”
"The current symptoms include _____________”
"Limited progress in ___________”
"Continues to be depressed as evidenced by ____________”
"Client continues to have suicidal ideation as evidenced by the following comment made
to this writer: ____________”
Who Relies On Your Documentation?
Clients’ Families
Rely on your documentation to advocate for the most appropriate and effective care
Physicians
Mental Health Professionals
Referral Sources
Rely on the medical record as an official and practical means of communicating with each other
Rely on your documentation to help them provide a unified treatment approach consistent with your work with the client
Rely on your documentation to provide continuity of care from one treatment setting to another
Employers
Other Payors
Managed Care Companies
Rely on your documentation to justify need for continued treatment, need for admission, demonstrate appropriateness and
Licensing and Accreditation Agencies
Rely on your documentation to verify your practice's quality of care and approve your license to operate
Chart Order
Left side
·Case Contact Summary Sheet
·Intake Form
·Client Information Questionnaire
·Release of Information Cover Letter
·Release of Information from Purdue Marriage and Family Therapy Center
·Informed Consent for Treatment
·Fee Contract
·Fee Receipts (balanced)
·Quality Assurance Review Sheets
Right side
·Treatment Plan (formulated by the 3rd session)
·Case Notes
·All drawings, correspondence, and other direct therapy documentation
·Termination/Transfer/Unopened Case Summaries
| Fact Name | Detail |
|---|---|
| Format Purpose | The DAP Note Sample form is designed to guide therapists in documenting client sessions effectively, focusing on data (D), assessment (A), and planning (P). |
| Content Structure | Each section of the note captures different elements: subjective and objective data fall under "D", observations and assessments under "A", and future plans under "P". |
| Legal Compliance | In states like California, the form should align with the California Business and Professions Code Section 4980.02 regarding the requirement for accurate and timely documentation. |
| Documentation Importance | Proper documentation is crucial for continuity of care and communication among healthcare providers, as it impacts treatment decisions and insurance reimbursements. |
Completing the DAP Note Sample form is a crucial part of documenting client interactions and progress. By following these instructions, you can ensure accurate and comprehensive record-keeping for therapy sessions.
Following these steps allows for effective documentation that reflects the therapeutic process. Always remember, clear and accurate notes serve both you and your clients throughout their therapeutic journey.
A DAP note is a structured format used by mental health professionals to document client interactions and progress. The acronym DAP stands for Data, Assessment, and Plan. This method helps therapists organize their notes in a clear and concise manner, ensuring all relevant information is included for ongoing care.
The DAP note consists of three main components:
The DAP note is structured to facilitate clear and effective documentation. Each section is clearly labeled, allowing therapists to input information consistently. For example, the Data section should reflect observations from the session, while the Assessment should summarize major points, and the Plan should specify upcoming actions. This format enhances communication and continuity of care.
Documenting client interactions serves multiple purposes. Primarily, it ensures that all stakeholders involved in the client’s care have access to necessary information. This documentation can advocate for treatment decisions, provide continuity of care, and meet legal and ethical requirements. Additionally, it helps the therapist track the client’s progress over time, adjusting treatment plans as needed.
To write effective DAP notes, consider the following best practices:
DAP notes provide a framework for identifying client needs, tracking behavioral changes, and evaluating progress. By using structured documentation, therapists can clearly see which strategies work effectively and which require adjustment. This objective data is crucial for creating a targeted treatment plan that evolves as the client progresses.
Multiple professionals utilize DAP notes within clinical settings. This includes therapists, counselors, psychiatrists, social workers, and other mental health professionals. By maintaining clear and detailed records, all members of the treatment team can provide coordinated care, enhancing the client’s overall experience.
Families, physicians, referral sources, and managed care companies often rely on DAP notes for various reasons. Families seek comprehensive documentation to advocate for a loved one's care. Physicians and mental health professionals use these notes for continuity and to align treatment protocols. Managed care companies may require detailed documentation to authorize continued sessions and support the cost-effectiveness of care.
When filling out the DAP Note Sample form, one of the common mistakes people make is not clearly distinguishing between subjective and objective data. The "D" section requires capturing both what the client says and what is observable by the therapist. Failing to include both can lead to incomplete notes that may not accurately reflect the session.
Another frequent error is neglecting to provide sufficient detail in the "A" assessment section. This section should analyze the situation by noting interventions and developing working hypotheses. If the assessment is vague, it may not give a clear picture of the client's progress or the therapist's insights.
Many people also fail to clearly outline the "P" response or plan. This section is vital for documenting what actions will be taken in future sessions. Without a specific plan, both the client and the therapist may feel uncertain about the next steps to take, leading to a lack of progress in therapy.
A significant mistake is overlooking the need to proofread the entries. Spelling or grammatical errors can distract from the content and undermine the professionalism of the documentation. Such oversights can cause confusion, especially if another professional references the notes.
People often leave blank spaces between entries, which can imply important information was omitted. Every entry should seamlessly connect to present a coherent narrative of the client's journey. Blank spaces can raise questions and detract from the clarity of the notes.
Utilizing abbreviations that are not universally recognized or approved also poses a problem. These abbreviations can create misunderstandings or misinterpretations of the notes, which could affect treatment decisions and care continuity.
Lastly, failing to document events chronologically can lead to a confusing record. Entries should be time-stamped correctly to maintain a clear timeline of the client's progress and therapeutic interventions. Inconsistent documentation can hinder effective communication among professionals who rely on accurate records for coordinated care.
When working with the DAP Note Sample form, several other documents and forms often accompany it in the treatment process. Each of these documents plays a crucial role in providing comprehensive care and maintaining effective communication between all parties involved. Here are four key forms frequently used alongside the DAP Note Sample form:
Together, these documents, along with the DAP Note Sample form, create a thorough framework for delivering effective therapy. By utilizing them, practitioners can ensure they are meeting the clients' needs while adhering to best practices in documentation and care coordination.
SOAP Notes: Similar to the DAP Note format, SOAP notes (Subjective, Objective, Assessment, Plan) provide a structured framework for documenting patient interactions, outlining what the patient reports, observations made during the session, assessments by the therapist, and plans for future sessions.
Progress Notes: Both DAP Notes and Progress Notes are used to track the client's progress over time. They include details about each session, what was discussed, and the client's development in treatment.
Case Management Notes: Like DAP Notes, these documents summarize interactions with clients and their current status in treatment, focusing on objectives and interventions needed for their care.
Client Treatment Plans: Both documents include goals and objectives tailored to the client’s needs. Treatment plans detail the therapeutic approach, while DAP Notes evaluate ongoing progress towards those aims.
Assessment Forms: DAP Notes share similarities with assessment forms, both aiming to capture the client's status and needs. Assessments often guide the therapist’s interventions, just as the DAP format outlines them clearly.
Contact Summaries: These records, like DAP Notes, document significant interactions with clients. They ensure continuity of care by summarizing important details and next steps after each session.
Informed Consent Forms: While informed consent focuses on what clients agree to in therapy, both forms are essential for documenting therapeutic processes, including client rights and treatment goals.
Referral Letters: Referral letters often summarize the client's situation and treatment needs. Similarly, DAP Notes outline the client's current issues and the interventions being employed, allowing for seamless continuity when transferred to another provider.
Supervision Notes: Like DAP Notes, supervision notes document therapy sessions but are specifically tailored to provide feedback and guidance for therapists under supervision regarding their case work.
Termination Summaries: These summaries, similar to DAP Notes, provide a comprehensive overview of the client's journey, summarizing their treatment, progress made, and any recommendations for future care as they prepare to conclude therapy.
When filling out the DAP Note Sample form, adhere to the following guidelines to ensure clarity and completeness.
Equally important are the practices to avoid when filling out the DAP Note Sample form:
Misconceptions about the DAP Note Sample form can lead to misunderstandings about its purpose and effectiveness. Here are some common myths, along with clarifications.
Understanding how to fill out and use the DAP Note Sample form is crucial for effective documentation in therapy sessions. Here are seven key takeaways to guide you: