The DCSS 0054 form is a crucial document for managing health insurance information related to child support arrangements in the state of California. It serves as a method for noncustodial parents to provide essential details regarding their health, dental, and vision insurance coverage. This information is not only pertinent to the custodial party but also plays a vital role in ensuring that children receive necessary medical care without financial strain. Section I of the form focuses on the health insurance provided by the noncustodial parent or their employer, prompting the disclosure of specific details such as the insurance company's name, policy numbers, and coverage amounts. Meanwhile, Section II addresses whether the other parent provides any health insurance, asking similar questions regarding their coverage. The final section, Section III, requires further confirmation of insurance status and guidance on notifying the local child support agency about the existence or absence of coverage. Overall, the DCSS 0054 form is an essential tool in facilitating communication between parents and local child support agencies, ensuring compliance with support obligations and the well-being of children involved.
STATE OF
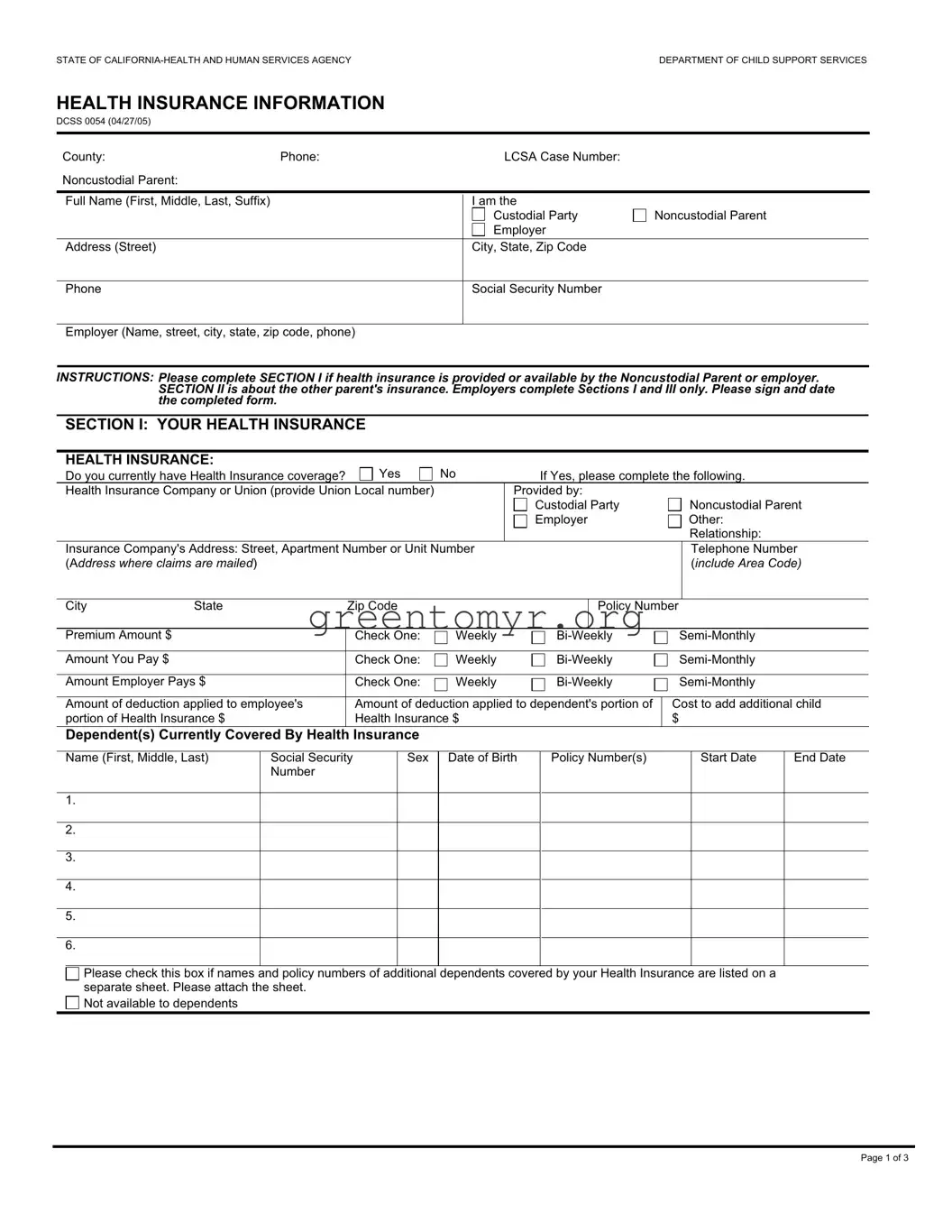
HEALTH INSURANCE INFORMATION
DCSS 0054 (04/27/05)
County: |
Phone: |
LCSA Case Number: |
|
Noncustodial Parent: |
|
|
|
|
|
|
|
Full Name (First, Middle, Last, Suffix) |
|
I am the |
|
|
|
Custodial Party |
Noncustodial Parent |
|
|
Employer |
|
Address (Street) |
|
City, State, Zip Code |
|
Phone
Social Security Number
Employer (Name, street, city, state, zip code, phone)
INSTRUCTIONS: Please complete SECTION I if health insurance is provided or available by the Noncustodial Parent or employer. SECTION II is about the other parent's insurance. Employers complete Sections I and III only. Please sign and date the completed form.
SECTION I: YOUR HEALTH INSURANCE
HEALTH INSURANCE:
Do you currently have Health Insurance coverage? |
Yes |
No |
If Yes, please complete the following. |
||||
Health Insurance Company or Union (provide Union Local number) |
|
Provided by: |
|
|
|||
|
|
|
|
Custodial Party |
|
Noncustodial Parent |
|
|
|
|
|
Employer |
|
Other: |
|
|
|
|
|
|
|
|
Relationship: |
Insurance Company's Address: Street, Apartment Number or Unit Number |
|
|
|
Telephone Number |
|||
(Address where claims are mailed) |
|
|
|
|
|
(include Area Code) |
|
|
|
|
|
|
|
|
|
City |
State |
Zip Code |
|
|
Policy Number |
||
|
|
|
|
|
|
|
|
Premium Amount $ |
|
Check One: |
Weekly |
||||
|
|
|
|
|
|
|
|
Amount You Pay $ |
|
Check One: |
Weekly |
||||
|
|
|
|
|
|
|
|
Amount Employer Pays $ |
Check One: |
Weekly |
|||||
|
|
|
|
|
|
||
Amount of deduction applied to employee's |
Amount of deduction applied to dependent's portion of |
Cost to add additional child |
|||||
portion of Health Insurance $ |
Health Insurance $ |
|
|
$ |
|
||
Dependent(s) Currently Covered By Health Insurance
|
Name (First, Middle, Last) |
Social Security |
Sex |
Date of Birth |
Policy Number(s) |
Start Date |
End Date |
|
|
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please check this box if names and policy numbers of additional dependents covered by your Health Insurance are listed on a separate sheet. Please attach the sheet.
Not available to dependents
Page 1 of 3
The Policy covers the following: (Check all that apply) |
|
|
|
Doctor Visits |
Medicare Supplemental |
Specific Illness |
Prescription Drugs |
Long Term Care |
Hospital Stays |
Hospital Outpatient |
Other (Specify): |
|
|
(i.e., lab work, physical therapy) |
|
DENTAL INSURANCE:
|
Do you currently have Dental Insurance coverage? |
Yes |
No |
|
|
If Yes, please complete the following. |
|
|
|||||||
|
Dental Insurance Company |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Dental Insurance Company's Address: Street, Apartment Number or Unit Number (address where claims are mailed) |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
State |
Zip Code |
|
|
|
|
Policy Number |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Premium Amount $ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Check One: |
Weekly |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Amount You Pay $ |
|
|
Check One: |
Weekly |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Amount Employer Pays $ |
|
|
Check One: |
Weekly |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Amount of deduction applied to employee's |
Amount of deduction applied to dependent's |
|
Cost to add additional child |
|||||||||||
|
portion of Health Insurance $ |
|
|
portion of health insurance $ |
|
$ |
|
|
|
|
|||||
|
Dependent(s) Covered by Dental Insurance |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Name (First, Middle, Last) |
|
Social Security |
Sex |
Date of Birth |
|
Policy Number(s) |
|
|
Start Date |
|
End Date |
|||
|
|
|
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please check this box if names and policy numbers of additional dependents covered by your Dental Insurance are listed on a separate sheet of paper. Please attach the sheet.
Not available to dependents
VISION INSURANCE:
Do you currently have Vision Insurance coverage? |
Yes |
No |
If Yes, please complete the following. |
Vision Insurance Company |
|
|
|
Vision Insurance Company's Address: Street, Apartment Number or Unit Number (Address where claims are mailed)
City |
State |
|
Zip Code |
|
|
Policy Number |
|
|
|
|
|
|
|
|
|
Premium Amount $ |
|
|
Check One: |
Weekly |
|||
|
|
|
|
|
|
|
|
Amount You Pay $ |
|
|
Check One: |
Weekly |
|||
Amount Employer Pays $ |
|
|
Check One: |
Weekly |
|||
|
|
|
|
|
|||
Amount of deduction applied to employee's |
Amount of deduction applied to dependent's portion |
Cost to add additional child |
|||||
portion of Health Insurance $ |
|
of health insurance $ |
|
|
|
$ |
|
Dependent(s) Covered by Vision Insurance
Name (First, Middle, Last) |
Social Security |
Sex |
|
Number |
|
1. |
|
|
|
|
|
2. |
|
|
|
|
|
3. |
|
|
|
|
|
4. |
|
|
|
|
|
5. |
|
|
|
|
|
6. |
|
|
|
|
|
Date of Birth
Policy Number(s)
Start Date
End Date
Please check this box if names and policy numbers of additional dependents covered by your Vision Insurance are listed on a separate sheet. Please attach the sheet.
Not available to dependents
HEALTH INSURANCE INFORMATION |
Page 2 of 3 |
|
|
DCSS 0054 (04/27/05) |
|
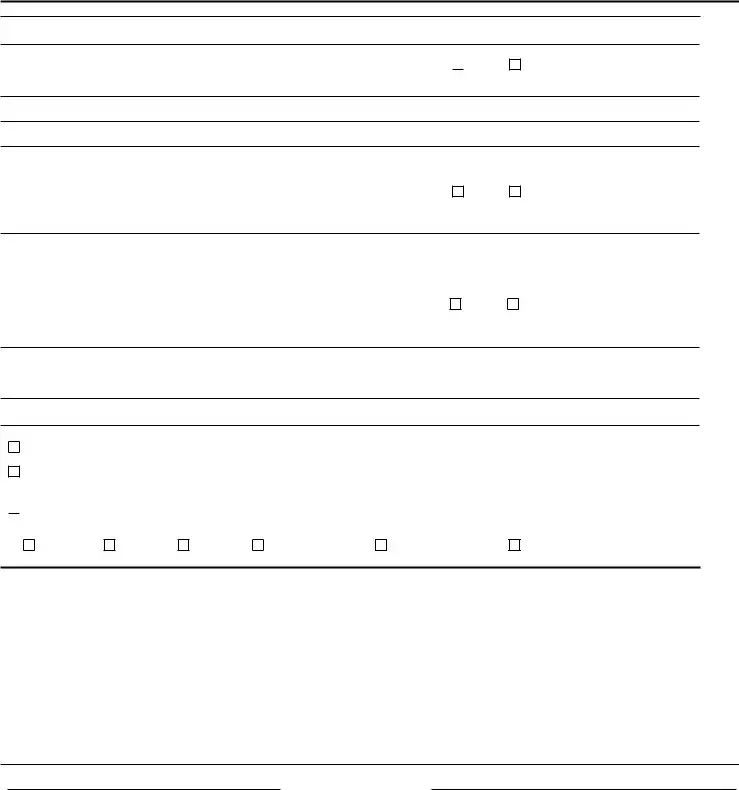
SECTION II: OTHER PARENT'S INSURANCE
HEALTH INSURANCE:
Does the other parent currently provide Health Insurance coverage for the child(ren) or you?  Yes If Yes, please complete the following information.
Yes If Yes, please complete the following information.
No
Health Insurance Company
Health insurance Company's Address: Street, Apartment Number or Unit Number (Address where claims are mailed)
City |
State |
Zip Code |
|
|
|
|
|
|
|
DENTAL INSURANCE: |
|
|
|
|
Does the other parent currently provide Dental Insurance coverage for the child(ren) or you? |
Yes |
No |
||
If Yes, please complete the following information. |
|
|
|
|
Dental Insurance Company |
|
|
|
|
Dental Insurance Company's Address: Street, Apartment Number or Unit Number (Address where claims are mailed)
City |
State |
Zip Code |
|
|
|
|
|
|
|
VISION INSURANCE: |
|
|
|
|
Does the other parent currently provide Vision Insurance coverage for the child(ren) or you? |
Yes |
No |
||
If Yes, please complete the following information. |
|
|
|
|
Vision Insurance Company |
|
|
|
|
Vision Insurance Company's Address: Street, Apartment Number or Unit Number (Address where claims are mailed)
City |
State |
Zip Code |
SECTION III: (MUST BE COMPLETED)
I have enclosed the insurance card(s)/information about the coverage for the child(ren).
At this time I do not have the insurance cards/information about the coverage for the child(ren). I will send the information to you when I get it from the insurance company.

 At this time there is no health insurance coverage available. I understand that if it becomes available, I will have to add my child(ren) onto the plan and then notify the local child support agency of the coverage. Coverage is unavailable because:
At this time there is no health insurance coverage available. I understand that if it becomes available, I will have to add my child(ren) onto the plan and then notify the local child support agency of the coverage. Coverage is unavailable because:
Not offered
Seasonal
Refused enrollment
Unreasonable in cost
Probationary period/date eligible
PRIVACY STATEMENT
The information Practices Act of 1997 (Civil Code Section 1798.17) and the Federal Privacy Act of 1974 (Public Law
Social Security Number information is mandatory and will be kept on file at the local child support agency to locate and identify individuals and assets for the purpose of establishing, modifying, and enforcing child support obligations. Enrolling a child in health insurance may require the release of the child's Social Security Number and mailing address to the other parent's employer or the release of the child's Social Security Number to the other parent.
The information in your case may be discussed with or given to the State, other agencies that can legally receive such information, and to the other parent or his/her attorney to the extent required by law.
SIGNATURE |
|
DATE |
|
|
|
|
|
|
|
|
PRINTED NAME |
TELEPHONE (include Area Code) |
|
|
|
|
|
|
|
|
TITLE |
|
|
|
|
|
|
|
|
HEALTH INSURANCE INFORMATION |
|
Page 3 of 3 |
|
|
DCSS 0054 (04/27/05) |
|
|
|
|
| Fact Name | Detail |
|---|---|
| Form Title | Health Insurance Information |
| Form Number | DCSS 0054 |
| Governing Law | California Family Code Section 4000 et seq. |
| Primary Purpose | To collect information regarding health insurance coverage for children involved in child support cases. |
| Completion Requirement | Sections I, II, and III must be completed by relevant parties to ensure proper documentation of insurance coverage. |
Filling out the DCSS 0054 form is essential for documenting health insurance information related to child support cases. After completing the form, you will submit it to the appropriate local child support agency. Ensure all information is accurate and complete to avoid delays in processing.
The DCSS 0054 form is a Health Insurance Information form used by the California Department of Child Support Services. It collects information about existing health, dental, and vision insurance coverage for children involved in child support cases. This ensures that both parents are informed about insurance options available for their children.
Both custodial and noncustodial parents may need to complete the form. If a noncustodial parent has health insurance or the employer provides it, Section I of the form must be filled out. Additionally, custodial parents must provide information regarding any other health insurance available for the child.
You will provide comprehensive details about health insurance coverage, including:
For dental and vision insurance, similar information is required. Fill out the sections relevant to your situation.
If you do not currently have health insurance available, you should indicate this on the form. You are also required to explain the reasons why coverage is unavailable. For instance, you might be unable to enroll due to costs, lack of availability, or a probationary period in your employment.
The form must be submitted whenever you receive a request from the local child support agency or when there is a change in health insurance coverage for your child. Timely submission ensures that the local agency can assist in keeping your child's insurance information up to date.
Your privacy is protected by law. The information collected in the DCSS 0054 form is used solely for purposes related to child support and is subject to strict confidentiality regulations. The Department of Child Support Services ensures compliance with privacy laws to keep your data secure.
When filling out the DCSS 0054 form, many individuals encounter common pitfalls that can lead to delays or complications in processing. One frequent mistake is leaving out essential information, particularly in the sections related to health insurance providers. If these fields are left blank, it may hinder the local child support agency's ability to verify coverage and communicate effectively.
Another common error involves misidentifying the noncustodial parent or custodial party. It’s crucial to ensure that the names are entered accurately as they appear on legal documents. An incorrect name can complicate the entire process, causing unnecessary confusion.
Many people also fail to provide complete addresses for health insurance companies and employers. The form requests specific details, such as the street address and zip code; omitting these can lead to delays since the agency may not be able to contact the relevant parties.
A significant oversight is not checking the appropriate boxes regarding existing insurance coverage. If you indicate "Yes" to having insurance when that's not accurate, it sets a false premise for further processing. Conversely, saying "No" when you do have coverage can have serious implications for support obligations.
Completing monetary fields incorrectly is another mistake often made. It's vital to accurately represent premium amounts and select the correct payment frequency. A discrepancy may lead to misunderstandings about financial responsibilities.
Failing to attach additional documents can also cause issues. If there are more dependents covered by your health insurance, make sure to include a separate sheet as requested. Not doing so can result in an incomplete submission, requiring follow-up.
In the section regarding the other parent's insurance, many individuals neglect to provide all required details or simply leave it blank. If the other parent has health insurance, it is necessary to fill in that information as it may affect support calculations.
Even minor mistakes, like writing illegibly or using the wrong format for dates, can complicate matters. Ensure that all entries are clear and conform to the specified formats to avoid confusion.
Additionally, forgetting to sign and date the form is a simple yet critical error. An unsigned form is often deemed invalid, necessitating a complete restart of the submission process.
Finally, individuals sometimes overlook important background information, such as the reason for lack of coverage, if applicable. This information can be pertinent and may influence future decisions regarding support and healthcare options.
The DCSS 0054 form plays a pivotal role in gathering health insurance information related to child support cases in California. Several other forms and documents can complement this form, ensuring a comprehensive understanding of a child's insurance coverage. Each of these documents serves a specific purpose, contributing to the overall complexity of child support and welfare cases.
Understanding these forms enhances one's ability to navigate the complexities of child support and health insurance requirements. It is crucial for all parties involved to be informed about the necessary documentation, as this can have a lasting impact on the welfare of the child and the financial responsibilities of the parents.
The DCSS 0054 form, which focuses on health insurance information for child support cases, has several similar documents that serve related purposes. Below is a list of these documents, each accompanied by a brief description of how they relate to the DCSS 0054 form.
Each of these documents plays a crucial role in the broader context of child support and health care provisions, reinforcing the importance of ensuring that children receive the necessary support and care.
When filling out the DCSS 0054 form, adhere to the following guidelines.
This form is necessary for both custodial and noncustodial parents. It collects information about health insurance coverage for children, which applies to both parties involved in child support agreements.
Filing the DCSS 0054 form is typically mandatory when health insurance is available. Failing to provide this information may affect child support calculations and obligations.
While the primary focus is on health insurance, the DCSS 0054 form also gathers details about dental and vision insurance coverage, ensuring comprehensive health support for the child.
Changes in insurance status, such as job changes or new coverage options, require updates to the DCSS 0054 form. Keeping this information current is crucial for accurate support and care decisions.
While privacy is a priority, certain details, especially Social Security Numbers, may be shared with relevant parties, including the other parent or their employer, as required by law.
Both parents must complete the necessary sections regarding their respective insurance coverage. This collaborative approach ensures that all potential sources of health care are considered for the child.
The DCSS 0054 form remains a vital part of the child support process. Despite being first issued in 2005, it continues to be relevant for parents navigating child support and health insurance obligations today.
When completing and using the DCSS 0054 form, it's important to follow certain guidelines to ensure that the process goes smoothly. Below are some key takeaways: