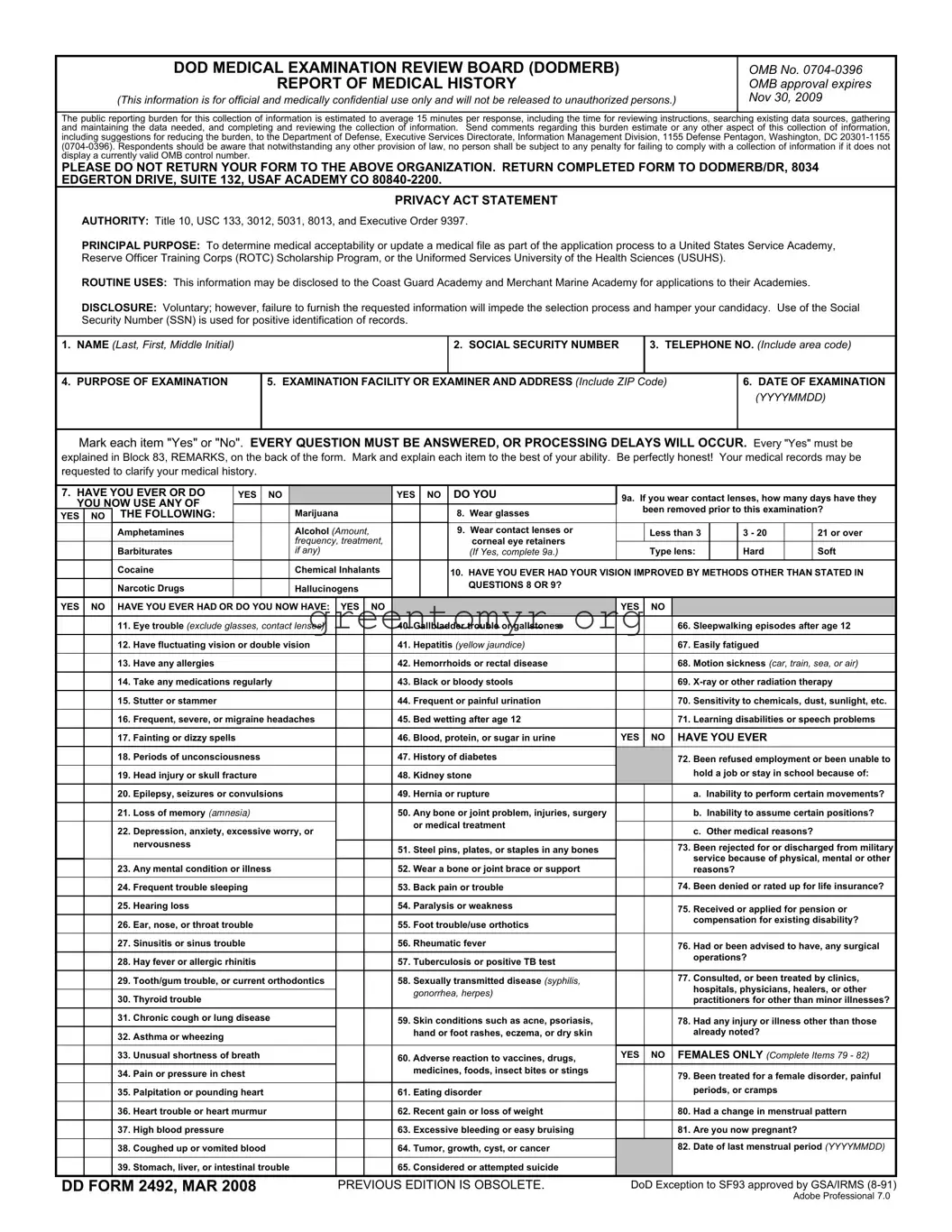
The DD 2492 form, also known as the Report of Medical History, plays a critical role in the evaluation process for individuals applying to prestigious military academies, ROTC scholarship programs, and the Uniformed Services University of the Health Sciences. Designed by the Department of Defense Medical Examination Review Board (DODMERB), this form collects comprehensive medical history to assess an applicant's medical acceptability. Applicants must provide personal information, including their name, Social Security number, and contact details, along with the specific purpose of the medical examination. The form requires a thorough and candid disclosure of past and present medical conditions, allergies, treatments, and medications, ensuring all questions are answered accurately to prevent processing delays. A notable feature is the disclosure of certain sensitive medical details, which must be clarified if marked "Yes" throughout the questionnaire. Additionally, it encompasses a privacy statement, emphasizing the importance of confidentiality. The responses not only inform medical personnel but also guide admissions decisions for the respective programs. Ultimately, the meticulous completion of this form directly influences an applicant's candidacy, making every detail crucial for a successful application. Moreover, the information, while voluntarily provided, is necessary for effective processing and timely evaluation. Applicants must be aware that omitting information may hinder their chances of success.
|
|
|
DOD MEDICAL EXAMINATION REVIEW BOARD (DODMERB) |
|
|
|
|
OMB No. |
||||||||||||||
|
|
|
|
|
|
|
REPORT OF MEDICAL HISTORY |
|
|
|
|
OMB approval expires |
||||||||||
|
|
(This information is for official and medically confidential use only and will not be released to unauthorized persons.) |
NOV 30, 2009 |
|||||||||||||||||||
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
The public reporting burden for this collection of information is estimated to average 15 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering |
||||||||||||||||||||||
and maintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information, |
||||||||||||||||||||||
including suggestions for reducing the burden, to the Department of Defense, Executive Services Directorate, Information Management Division, 1155 Defense Pentagon, Washington, DC |
||||||||||||||||||||||
display a currently valid OMB control number. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
PLEASE DO NOT RETURN YOUR FORM TO THE ABOVE ORGANIZATION. RETURN COMPLETED FORM TO DODMERB/DR, 8034 |
||||||||||||||||||||||
EDGERTON DRIVE, SUITE 132, USAF ACADEMY CO |
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
PRIVACY ACT STATEMENT |
|
|
|
|
|
|
|
|
|||
|
AUTHORITY: Title 10, USC 133, 3012, 5031, 8013, and Executive Order 9397. |
|
|
|
|
|
|
|
|
|||||||||||||
|
PRINCIPAL PURPOSE: To determine medical acceptability or update a medical file as part of the application process to a United States Service Academy, |
|||||||||||||||||||||
|
Reserve Officer Training Corps (ROTC) Scholarship Program, or the Uniformed Services University of the Health Sciences (USUHS). |
|
|
|
|
|||||||||||||||||
|
ROUTINE USES: This information may be disclosed to the Coast Guard Academy and Merchant Marine Academy for applications to their Academies. |
|
||||||||||||||||||||
|
DISCLOSURE: Voluntary; however, failure to furnish the requested information will impede the selection process and hamper your candidacy. Use of the Social |
|||||||||||||||||||||
|
Security Number (SSN) is used for positive identification of records. |
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
1. NAME (Last, First, Middle Initial) |
|
|
|
|
|
|
|
|
|
2. SOCIAL SECURITY NUMBER |
|
3. TELEPHONE NO. (Include area code) |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
4. PURPOSE OF EXAMINATION |
|
|
5. EXAMINATION FACILITY OR EXAMINER AND ADDRESS (Include ZIP Code) |
6. DATE OF EXAMINATION |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(YYYYMMDD) |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Mark each item "Yes" or "No". EVERY QUESTION MUST BE ANSWERED, OR PROCESSING DELAYS WILL OCCUR. Every "Yes" must be |
||||||||||||||||||||||
explained in Block 83, REMARKS, on the back of the form. Mark and explain each item to the best of your ability. Be perfectly honest! Your medical records may be |
||||||||||||||||||||||
requested to clarify your medical history. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
7. HAVE YOU EVER OR DO |
|
YES |
|
NO |
|
|
|
YES |
NO |
DO YOU |
9a. If you wear contact lenses, how many days have they |
|||||||||||
YOU NOW USE ANY OF |
|
|
|
|
Marijuana |
|
|
|
8. Wear glasses |
|
been removed prior to this examination? |
|||||||||||
YES |
NO |
THE FOLLOWING: |
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
Amphetamines |
|
|
|
|
Alcohol (Amount, |
|
|
|
9. Wear contact lenses or |
|
Less than 3 |
|
3 - 20 |
|
|
21 or over |
||||
|
|
|
|
|
|
|
|
frequency, treatment, |
|
|
|
corneal eye retainers |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Barbiturates |
|
|
|
|
if any) |
|
|
|
(If Yes, complete 9a.) |
|
Type lens: |
|
Hard |
|
|
Soft |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cocaine |
|
|
|
|
Chemical Inhalants |
|
|
|
10. HAVE YOU EVER HAD YOUR VISION IMPROVED BY METHODS OTHER THAN STATED IN |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
Narcotic Drugs |
|
|
|
|
Hallucinogens |
|
|
|
QUESTIONS 8 OR 9? |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
YES |
NO |
HAVE YOU EVER HAD OR DO YOU NOW HAVE: |
YES |
NO |
|
|
|
|
YES |
NO |
|
|
|
|
|
|
||||||
|
|
11. |
Eye trouble (exclude glasses, contact lenses) |
|
|
40. |
Gallbladder trouble or gallstones |
|
|
66. Sleepwalking episodes after age 12 |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
12. |
Have fluctuating vision or double vision |
|
|
41. |
Hepatitis (yellow jaundice) |
|
|
67. Easily fatigued |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
13. |
Have any allergies |
|
|
|
|
|
|
42. |
Hemorrhoids or rectal disease |
|
|
68. Motion sickness (car, train, sea, or air) |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
14. |
Take any medications regularly |
|
|
43. |
Black or bloody stools |
|
|
69. |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
15. |
Stutter or stammer |
|
|
|
|
|
|
44. |
Frequent or painful urination |
|
|
70. Sensitivity to chemicals, dust, sunlight, etc. |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
16. |
Frequent, severe, or migraine headaches |
|
|
45. |
Bed wetting after age 12 |
|
|
71. Learning disabilities or speech problems |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
17. |
Fainting or dizzy spells |
|
|
|
|
|
|
46. |
Blood, protein, or sugar in urine |
YES |
NO |
HAVE YOU EVER |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. |
Periods of unconsciousness |
|
|
|
|
47. |
History of diabetes |
|
|
72. Been refused employment or been unable to |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
19. |
Head injury or skull fracture |
|
|
|
|
48. |
Kidney stone |
|
|
hold a job or stay in school because of: |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
20. |
Epilepsy, seizures or convulsions |
|
|
49. |
Hernia or rupture |
|
|
a. Inability to perform certain movements? |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
21. |
Loss of memory (AMNESIA) |
|
|
|
|
50. |
Any bone or joint problem, injuries, surgery |
|
|
b. Inability to assume certain positions? |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
or medical treatment |
|
|
|
|
|
|
|
|
||
|
|
22. |
Depression, anxiety, excessive worry, or |
|
|
|
|
|
c. Other medical reasons? |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
nervousness |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
51. |
Steel pins, plates, or staples in any bones |
|
|
73. Been rejected for or discharged from military |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
service because of physical, mental or other |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
23. |
Any mental condition or illness |
|
|
52. |
Wear a bone or joint brace or support |
|
|
|||||||||||||
|
|
|
|
|
|
reasons? |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
24. |
Frequent trouble sleeping |
|
|
|
|
53. |
Back pain or trouble |
|
|
74. Been denied or rated up for life insurance? |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
25. |
Hearing loss |
|
|
|
|
|
|
54. |
Paralysis or weakness |
|
|
75. Received or applied for pension or |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
26. |
Ear, nose, or throat trouble |
|
|
|
|
55. |
Foot trouble/use orthotics |
|
|
compensation for existing disability? |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
27. |
Sinusitis or sinus trouble |
|
|
|
|
56. |
Rheumatic fever |
|
|
76. Had or been advised to have, any surgical |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
28. |
Hay fever or allergic rhinitis |
|
|
|
|
57. |
Tuberculosis or positive TB test |
|
|
operations? |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
29. |
Tooth/gum trouble, or current orthodontics |
|
|
58. |
Sexually transmitted disease (syphilis, |
|
|
77. Consulted, or been treated by clinics, |
||||||||||||
|
|
|
|
|
|
hospitals, physicians, healers, or other |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
gonorrhea, herpes) |
|
|
||||||||
|
|
30. |
Thyroid trouble |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
practitioners for other than minor illnesses? |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
31. |
Chronic cough or lung disease |
|
|
59. |
Skin conditions such as acne, psoriasis, |
|
|
78. Had any injury or illness other than those |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
32. |
Asthma or wheezing |
|
|
|
|
|
|
|
hand or foot rashes, eczema, or dry skin |
|
|
already noted? |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
33. |
Unusual shortness of breath |
|
|
|
|
60. |
Adverse reaction to vaccines, drugs, |
YES |
NO |
FEMALES ONLY (Complete Items 79 - 82) |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
34. |
Pain or pressure in chest |
|
|
|
|
|
medicines, foods, insect bites or stings |
|
|
79. Been treated for a female disorder, painful |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
35. |
Palpitation or pounding heart |
|
|
|
|
61. |
Eating disorder |
|
|
periods, or cramps |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
36. |
Heart trouble or heart murmur |
|
|
|
|
62. |
Recent gain or loss of weight |
|
|
80. Had a change in menstrual pattern |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
37. |
High blood pressure |
|
|
|
|
|
|
63. |
Excessive bleeding or easy bruising |
|
|
81. Are you now pregnant? |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
38. |
Coughed up or vomited blood |
|
|
|
|
64. |
Tumor, growth, cyst, or cancer |
|
|
82. Date of last menstrual period (YYYYMMDD) |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
39. |
Stomach, liver, or intestinal trouble |
|
|
65. |
Considered or attempted suicide |
|
|
|
|
|
|
|
|
|||||||
DD FORM 2492, MAR 2008 |
|
|
PREVIOUS EDITION IS OBSOLETE. |
DoD Exception to SF93 approved by GSA/IRMS |
||||||||||||||||||
Adobe Professional 7.0
83.REMARKS. Applicant use only. Every "yes" response in items 7 through 81 must be explained in the space provided. Give specific dates and details including names of physicians and hospitals or clinics and the current status of the condition. If additional space is required, continue on a separate sheet and attach to this form.
84.CERTIFICATION. I certify that I have reviewed the foregoing information supplied by me and that it is true and complete to the best of my knowledge. I authorize any of the physicians, hospitals, or clinics mentioned above to furnish the Government a complete transcript of my medical record for purposes of processing my application for this employment or service.
TYPED OR PRINTED NAME OF EXAMINEE/APPLICANT
SIGNATURE OF EXAMINEE/APPLICANT
DATE SIGNED
(YYYYMMDD)
85.EXAMINER'S SUMMARY AND ELABORATION OF ALL PERTINENT DATA. Examiner shall comment on all "Yes" and blank answers, indicating the item number before each comment. Develop by interview any additional medical history deemed important, and record significant findings here. If additional space is required, continue on a separate sheet and attach to this form.
86. EXAMINER
TYPED OR PRINTED NAME OF EXAMINER
SIGNATURE OF EXAMINER
DATE SIGNED
(YYYYMMDD)
87.NUMBER OF ATTACHED SHEETS
DD FORM 2492 (BACK), MAR 2008
| Fact Name | Details |
|---|---|
| Purpose | The DD Form 2492 is used to evaluate the medical acceptability of candidates applying to service academies and ROTC programs. |
| Privacy Act Statement | Information collected is confidential and will not be disclosed improperly. Sharing your Social Security Number helps ensure accurate record-keeping. |
| Completion Requirement | All questions must be answered entirely. Incomplete forms can cause processing delays, so honesty is crucial. |
| Return Instructions | Completed forms should not be sent to the OMB but directly to DODMERB at the specified address in Colorado. |
Completing the DD Form 2492 is an important step in the application process for various military programs. It's essential to be meticulous and truthful while filling out the form since accurate information helps in assessing your medical history for eligibility. Here are the steps to guide you through the process:
The DD Form 2492 is used to report medical history for individuals applying to a United States Service Academy, Reserve Officer Training Corps (ROTC) Scholarship Program, or the Uniformed Services University of the Health Sciences (USUHS). It helps assess medical acceptability and keeps your medical file updated.
This form must be completed by applicants who are seeking entry into military service academies, programs for ROTC scholarships, or specific universities dedicated to health sciences. If you are applying to any of these institutions, it's essential to provide accurate information on this form.
Completing the DD Form 2492 accurately is crucial. If you fail to answer all questions or provide incomplete information, it could lead to processing delays. Additionally, omitting details might hinder your admissions process, as it impedes your candidacy.
If you check "Yes" on any health-related questions, you must provide a detailed explanation in Block 83 of the form. Include specific dates, conditions, treatment information, and names of healthcare providers or facilities. This transparency is necessary for a comprehensive medical evaluation.
Completing the DD 2492 form can be a crucial step for individuals involved in military applications. However, many make common mistakes that can lead to delays or complications in their applications. Being aware of these pitfalls can save time and reduce stress during the process.
One frequent mistake occurs when applicants fail to answer every question on the form. The instructions clearly state that "every question must be answered." Leaving any question blank might slow down the processing time of your application. It's essential to take the time to read through each question carefully and provide an answer, even if you feel the question isn't applicable to your situation.
Another common error is not providing sufficient detail in the remarks section for any "Yes" answers. For instance, if you indicate a history of a particular condition, you must elaborate on it in Block 83. This includes dates, involved healthcare providers, and the current status of the condition. Neglecting to provide thorough explanations can lead to misunderstandings or even result in the application being denied due to perceived lack of transparency.
A third mistake involves incorrect or incomplete personal information, such as your name or Social Security number. Double-checking this data is essential. Errors in this area can lead to misidentification and can create significant delays in processing your application. The form's confidentiality emphasizes the importance of providing accurate information every step of the way.
Finally, applicants often rush to submit the form without reviewing it thoroughly. This hurried approach can lead to multiple errors, which may seem minor but can have a cumulative effect on the outcome of your application. Taking a few extra minutes to read through your entries and ensure clarity can make a substantial difference in the processing timeline and the overall success of the application.
The DD 2492 form serves as a report of medical history that is part of the assessment process for applicants to military academies and related programs. Several other forms and documents may accompany it to provide comprehensive information about the applicant's medical status. Below is a list of nearly nine common documents often used in conjunction with the DD 2492 form, each identified by its purpose in the application process.
These documents each play a vital role in ensuring that all necessary medical information is available for review. Together, they help streamline the evaluation process and contribute to the applicant's understanding of their medical standing in relation to military service.
When filling out the DD 2492 form, accuracy and honesty are essential. Below are ten tips outlining what you should do and what you should avoid.
By adhering to these guidelines, you can ensure that your submission is clear and complete, which increases your chances of prompt processing.
The DD Form 2492 is an essential document in the military application process, particularly for those interested in service academies or ROTC programs. However, several misconceptions exist regarding its purpose and requirements. Below are five common misconceptions, along with clarifications:
Understanding these misconceptions is vital for anyone navigating the application process. Accurate completion of the DD Form 2492 informs military officials about one's medical history, allowing for a fair review of eligibility based on both physical and mental wellness.
The DD 2492 form is essential for applicants to U.S. Service Academies and ROTC programs. Understanding the process of filling it out can make a significant difference in your application experience.
Using the DD 2492 form accurately and thoroughly will facilitate a smooth examination process, preventing potential setbacks in your application journey.