The DD 2870 form is an essential document utilized primarily in the United States military and various branches of the Department of Defense. It serves as the "Authorization for Disclosure of Medical or Dental Information," allowing service members and veterans to grant permission for their medical information to be shared with specific individuals or entities. The completion of this form is often necessary for obtaining medical treatment, transferring care, or even accessing disability benefits. Military personnel may use the DD 2870 to authorize the release of their medical records to healthcare providers, family members, or legal representatives. Understanding the proper use of this form is crucial, as it helps protect an individual's privacy while ensuring that necessary information is accessible for care and support. Additionally, specific instructions regarding the completion of the form, the parties involved, and the duration of the authorization are critical components that individuals must consider before submission. Compliance with the guidelines outlined in the DD 2870 form ensures that all parties respect the confidentiality of the service member's health information, aligning with both military regulations and privacy laws.
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
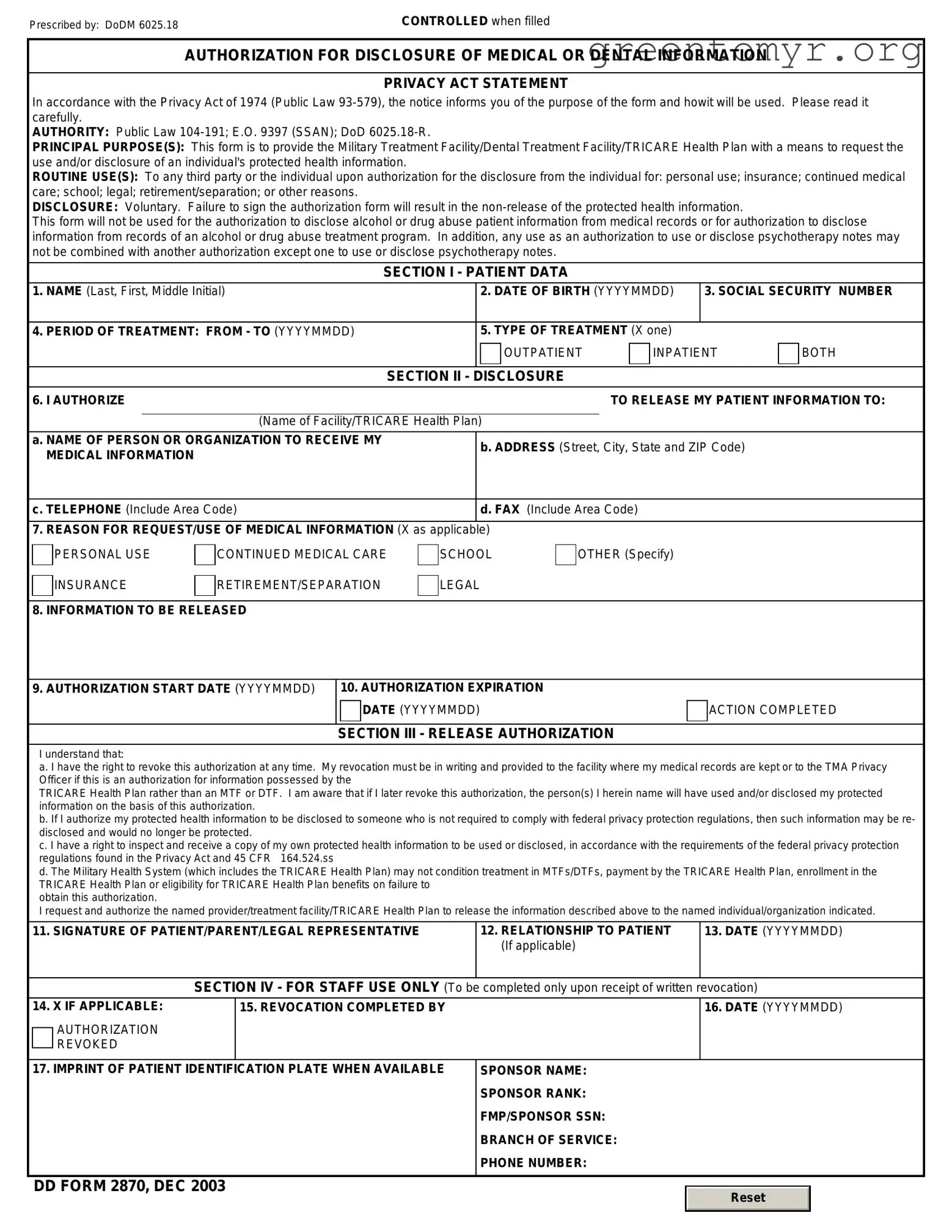
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
| Fact Name | Description |
|---|---|
| Purpose | The DD 2870 form is used to request access to a service member's military medical records and information from the Department of Defense. |
| Eligibility | Eligible individuals include service members, their authorized representatives, or legally-designated representatives. |
| Governing Regulations | The use of the DD 2870 form is governed by the Freedom of Information Act (FOIA) and Department of Defense (DoD) regulations. |
| Submission Process | After completing the form, it must be submitted to the appropriate military branch's records custodian. |
| Processing Time | Requests typically take 10 to 20 business days for processing, but may vary depending on the volume of requests. |
The DD 2870 form is a vital document in certain military processes. After completion, the form needs to be submitted to the appropriate authorities for processing. This submission may lead to access to services or benefits as indicated by the form's purpose.
The DD 2870 form is a document used by military service members, their families, and eligible beneficiaries to authorize the release of medical information. It ensures that individuals consent to have their medical records shared as necessary for their care and administrative purposes.
This form is typically completed by service members or their authorized representatives when they need to allow healthcare providers or other entities access to their medical information. It's particularly relevant during transitions between healthcare systems or in legal situations involving medical records.
The DD 2870 form requests various pieces of information, including:
Once completed, the DD 2870 form should be submitted to the appropriate medical facility or organization that will process the request. It may require either physical delivery or electronic submission, depending on the facility's protocols.
Yes, individuals have the right to revoke their consent at any time. To do this, a written notice of revocation should be provided to the organization that received the original consent. It is important to include identifying information to ensure the correct record is updated.
The authorization provided by the DD 2870 form remains valid until it is revoked or until the specific time frame indicated in the document expires. Individuals should review and update their authorization as necessary to reflect their current preferences.
The DD 2870 form can typically be found on official military or government websites. It is recommended to visit the Defense Health Agency or similar resources where military-related documents are hosted to download and print the form.
Filling out the DD 2870 form can be a straightforward process, but there are common errors that individuals may encounter. One mistake often seen is the failure to provide accurate personal information. This includes not entering the correct Social Security number or misrepresenting addresses. Such inaccuracies can lead to complications down the line, resulting in delays and possibly affecting benefits.
Another frequent mistake is not signing the form. Without a signature, the form is incomplete and cannot be processed. Many people forget this step, especially if they are in a rush to submit their paperwork. Ensuring that all required signatures are included is crucial for timely handling of the application.
Some applicants neglect to check the instructions carefully. The DD 2870 comes with specific guidelines on how to fill it out, including which documents or additional information may be required. Ignoring these instructions can lead to omitted information, which might result in the form being returned or denied.
Providing insufficient detail in the sections that require explanations is another common misstep. Applicants sometimes write vague answers or leave portions blank when prompted for thorough explanations. Offering comprehensive, clear responses helps the reviewing agency fully understand the applicant's situation.
Moreover, individuals often fail to double-check for typos or formatting issues before submission. Small errors, like misspellings of names or incorrect dates, can create confusion and hinder the processing of the form. Taking the time to proofread can prevent these easily avoidable mistakes.
Lastly, individuals may overlook the submission deadline. Each application has a specific timeline in which it must be submitted. Missing this deadline can result in the loss of benefits or additional complications. Being aware of and adhering to deadlines is essential for the successful completion of the process.
The DD 2870 form, officially known as the "Authorization for Disclosure of Medical or Dental Information," facilitates the release of medical information by the U.S. Department of Defense. When submitting this form, individuals may need to accompany it with several other documents to ensure a comprehensive application. Below is a list of related forms and documents often used in conjunction with the DD 2870 form, along with brief descriptions of each. These documents help streamline processes and clarify requests for medical or dental information.
Completing and submitting the DD 2870 form alongside these associated documents can facilitate a smoother process in obtaining relevant medical or dental information. Whether you are a veteran, a family member, or a legal representative, understanding these forms ensures that you can navigate the system effectively.
The DD 2870 form is a widely used document within the military context, particularly for those seeking to access their medical records or related health information. Several other documents serve a similar purpose in facilitating access to sensitive information or conveying consent. Below are four documents that share similarities with the DD 2870 form:
When filling out the DD 2870 form, it is important to follow certain guidelines to ensure accuracy and efficiency. Here are seven things to do and not to do:
The DD 2870 form, known as the "Authorization for Disclosure of Medical or Dental Information," often leads to misunderstandings. Here are nine common misconceptions regarding this important document.
Being aware of these misconceptions can help alleviate concerns and ensure that the DD 2870 form is used correctly and effectively when needed.
The DD 2870 form is essential for requesting military health care benefits and services. Here are some key takeaways to help you navigate filling it out and using it effectively.
Understanding these key elements of the DD 2870 form can streamline your experience in accessing military health care benefits.
Boe 245 Oye - Incorrect or missing information can significantly delay the processing timeline.
Annual Report Format - Tennessee Corporation Annual Report Form is essential for compliance.
Alabama Secure Power of Attorney - The MC-25 can be particularly advantageous when dealing with out-of-state vehicle transactions or services.