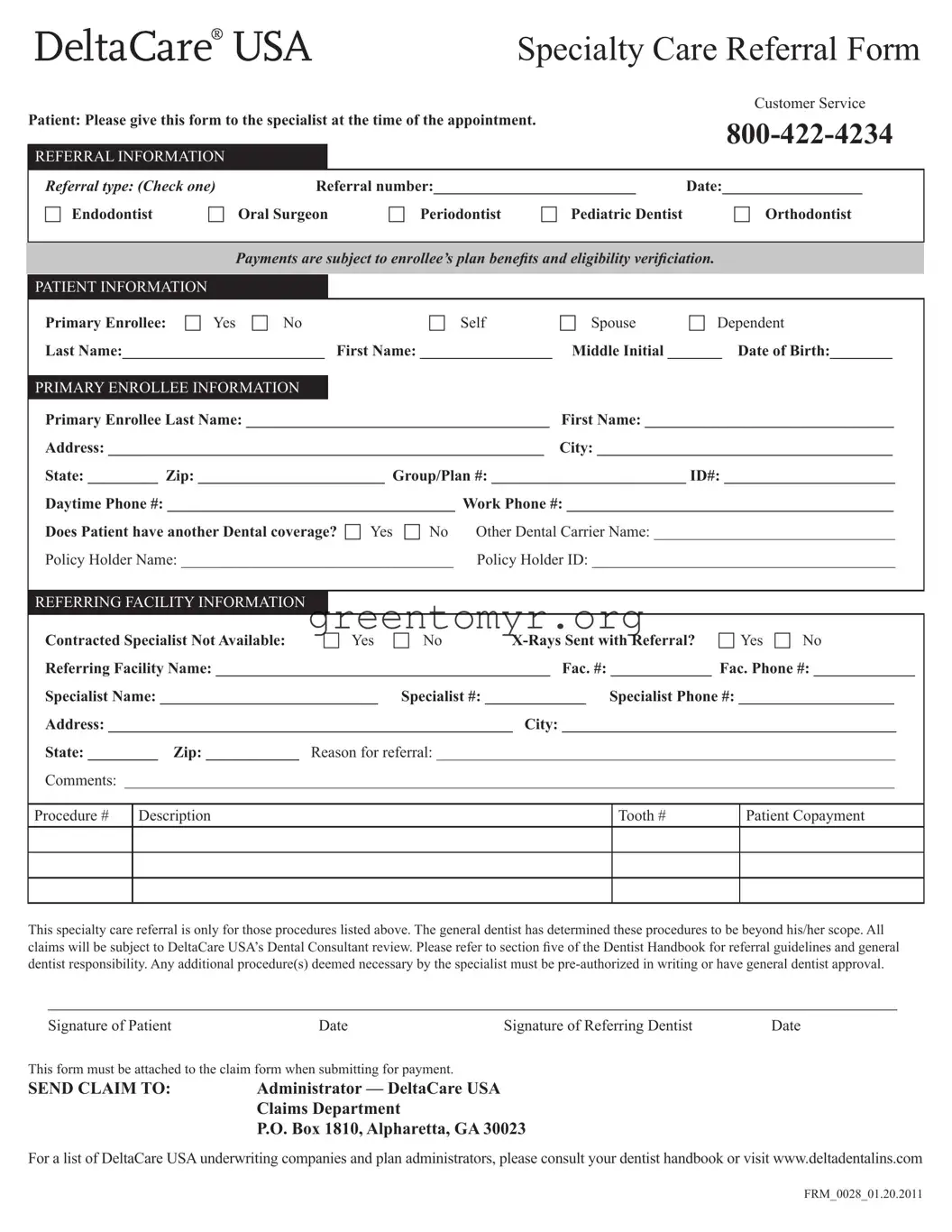
The Deltacare USA form serves as a critical tool for ensuring patients receive appropriate specialty dental care while adhering to the guidelines set forth by DeltaCare USA. This form must be completed by the referring general dentist and presented to the specialist at the time of the appointment. It includes essential information such as the type of referral—options range from endodontists to orthodontists—and requires specific details about the patient and the primary enrollee, including their personal information and insurance coverage. If the patient has an existing dental plan besides DeltaCare, that information must also be documented. Additionally, the form requests details about the referring facility and specialist, alongside a clear indication of whether X-rays accompany the referral. Importantly, the Deltacare USA form emphasizes that all procedures requiring specialist intervention must be pre-authorized or approved by the general dentist. Because the general dentist's expertise determines whether a referral is necessary, this process safeguards the integrity of patient treatment while overseeing costs associated with specialty claims. Understanding the nuances of this form is imperative for both patients seeking specialized care and the healthcare professionals responsible for their treatment.
Specialty Care Referral Form
|
|
|
|
|
|
Customer Service |
Patient: Please give this form to the specialist at the time of the appointment. |
|
|||||
|
|
|
|
|
|
|
REFERRAL INFORMATION |
|
|
|
|
|
|
|
|
|
|
|||
Referral type: (Check one) |
Referral number:__________________________ |
Date:__________________ |
||||
c Endodontist |
c Oral Surgeon |
c Periodontist |
c Pediatric Dentist |
c Orthodontist |
||
|
|
|
|
|
|
|
Payments are subject to enrollee’s plan beneits and eligibility veriiciation.
PATIENT INFORMATION
Primary Enrollee: c Yes c No |
c Self |
c Spouse |
c Dependent |
Last Name:__________________________ |
First Name: _________________ |
Middle Initial _______ Date of Birth:________ |
|
|
|
|
|
PRIMARY ENROLLEE INFORMATION |
|
|
|
Primary Enrollee Last Name: _______________________________________ |
First Name: ________________________________ |
||
Address: ________________________________________________________ |
City: ______________________________________ |
||
State: _________ Zip: ________________________ Group/Plan #: _________________________ ID#: ______________________
Daytime Phone #: _____________________________________ Work Phone #: __________________________________________
Does Patient have another Dental coverage? c Yes |
c No |
Other Dental Carrier Name: _______________________________ |
|
Policy Holder Name: ___________________________________ |
Policy Holder ID: _______________________________________ |
||
|
|
|
|
REFERRING FACILITY INFORMATION |
|
|
|
|
|
|
|
Contracted Specialist Not Available: |
c Yes |
c No |
|
Referring Facility Name: ___________________________________________ Fac. #: _____________ Fac. Phone #: _____________
Specialist Name: ____________________________ Specialist #: _____________ Specialist Phone #: ____________________
Address: ____________________________________________________ City: ___________________________________________
State: _________ Zip: ____________ Reason for referral: ___________________________________________________________
Comments: ___________________________________________________________________________________________________
Procedure # |
Description |
Tooth # |
Patient Copayment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
This specialty care referral is only for those procedures listed above. The general dentist has determined these procedures to be beyond his/her scope. All
claims will be subject to DeltaCare USA’s Dental Consultant review. Please refer to section ive of the Dentist Handbook for referral guidelines and general
dentist responsibility. Any additional procedure(s) deemed necessary by the specialist must be
___________________________________________________________________________________________
Signature of Patient |
Date |
Signature of Referring Dentist |
Date |
This form must be attached to the claim form when submitting for payment.
SEND CLAIM TO: |
Administrator — DeltaCare USA |
|
Claims Department |
|
P.O. Box 1810, Alpharetta, GA 30023 |
For a list of DeltaCare USA underwriting companies and plan administrators, please consult your dentist handbook or visit www.deltadentalins.com
FRM_0028_01.20.2011
| Fact Name | Details |
|---|---|
| Referral Purpose | This form is used to request a referral to a dental specialty provider, ensuring that patients receive appropriate care for complex procedures. |
| Patient Instructions | Patients must present this form to the specialist at their appointment to ensure the referral process runs smoothly. |
| Appointment Type | Patients need to indicate the type of referral by checking the appropriate box for the specialty required, such as endodontist or orthodontist. |
| Primary Enrollee Information | Complete information about the primary enrollee is requested, including name, address, and contact details to verify eligibility. |
| Co-Payment Information | Patients are advised that copayments are dependent on their specific dental plan benefits and must be verified. |
| Claim Submission Requirement | The completed form must accompany any claims submitted for payment to DeltaCare USA’s Claims Department. |
| State-Specific Law | Depending on the state, laws related to dental referrals and coverage eligibility may apply. Always check local regulations. |
Filling out the Deltacare USA form is an important step for patients requiring specialty dental care. This document needs to be completed accurately and presented to the specialist at the time of your appointment. Below are the steps to guide you through the process.
Don't forget to attach this form to the claim form when you're ready to submit for payment. It’s important to follow these steps closely to ensure a smooth process for your dental care needs.
The Deltacare USA form serves as a Specialty Care Referral Form. It allows patients to obtain approval for specialized dental procedures beyond what a general dentist can provide. Patients must present this form to the specialist at the time of their appointment.
To complete the form, follow these steps:
The form allows referrals to several specialties, including:
You will need to provide the following patient information:
If the contracted specialist is not available, indicate this by checking the "Contracted Specialist Not Available" box on the form. The form should then be completed as much as possible. Additional steps may be needed to find an alternative specialist.
If the specialist identifies additional procedures that are necessary, they must obtain pre-authorization in writing or seek approval from the general dentist. This ensures that all actions comply with DeltaCare USA's guidelines.
Once the form is completed and signed, it must be attached to the claim form. Submit the claim to:
Administrator — DeltaCare USA Claims Department
P.O. Box 1810
Alpharetta, GA 30023
If the patient has other dental insurance, it's important to provide that information on the form. This includes the name of the other carrier and the policyholder's details. This information helps ensure that claims are processed accurately and efficiently.
For additional details regarding DeltaCare USA's guidelines, underwriting companies, or plan administrators, consult your dentist handbook or visit www.deltadentalins.com .
When filling out the Deltacare USA form, several common mistakes can occur, potentially leading to delays or issues with processing the referral. One of the most frequent errors is failing to check the correct referral type. It’s crucial to tick the appropriate box for the type of specialist being referred to, as this categorization ensures that the patient receives appropriate care.
Another common mistake is incomplete patient information. All fields must be accurately completed, including the patient's last name, first name, and date of birth. Omitting this information could lead to difficulties in verifying patient eligibility and processing the referral.
Additionally, many individuals overlook the importance of verifying the primary enrollee’s information. It’s essential to ensure that the enrollee’s details, including name and ID number, match those on the insurance plan. Discrepancies can cause delays in claims processing.
Another area where mistakes frequently occur is under the section regarding other dental coverage. Individuals should clearly indicate whether they have additional dental insurance, providing the name of the carrier and policy holder if applicable. Failure to disclose this information can affect claim approvals.
Providing accurate phone numbers is also often neglected. Users should ensure that the daytime and work phone numbers are correct and accessible. Incorrect contact information can impede communication between the dental office and the patient.
Furthermore, not attaching the referral form to the claim form when submitting for payment is a critical oversight. This step is essential for the claims department to review the referral and process payments accurately.
Lastly, it is vital to understand the requirements for additional procedures. Patients must remember that any new treatments suggested by the specialist need prior authorization. This stipulation is necessary to prevent potential payment disputes.
The Deltacare USA form is used for referrals related to specialty dental care. Several other documents often accompany this form to ensure smooth processing and clarity of information about the patient's care and coverage. The following is a list of related forms and documents that may be required or beneficial during the referral and claims process.
These documents work together with the Deltacare USA form to streamline the referral and claims process for dental care. Ensuring all necessary forms are completed and submitted can aid in the efficient processing of claims and enhance communication among all parties involved in patient care.
When filling out the DeltaCare USA form, consider the following important points:
Many individuals hold misconceptions about the DeltaCare USA form, which can lead to confusion and delays in receiving care. Below is a list of five common misconceptions:
Understanding these misconceptions will help ensure a smoother experience when navigating dental care with DeltaCare USA.
When filling out the Deltacare USA form, keep these key takeaways in mind:
Following these steps will help ensure a smooth process when using the Deltacare USA form.