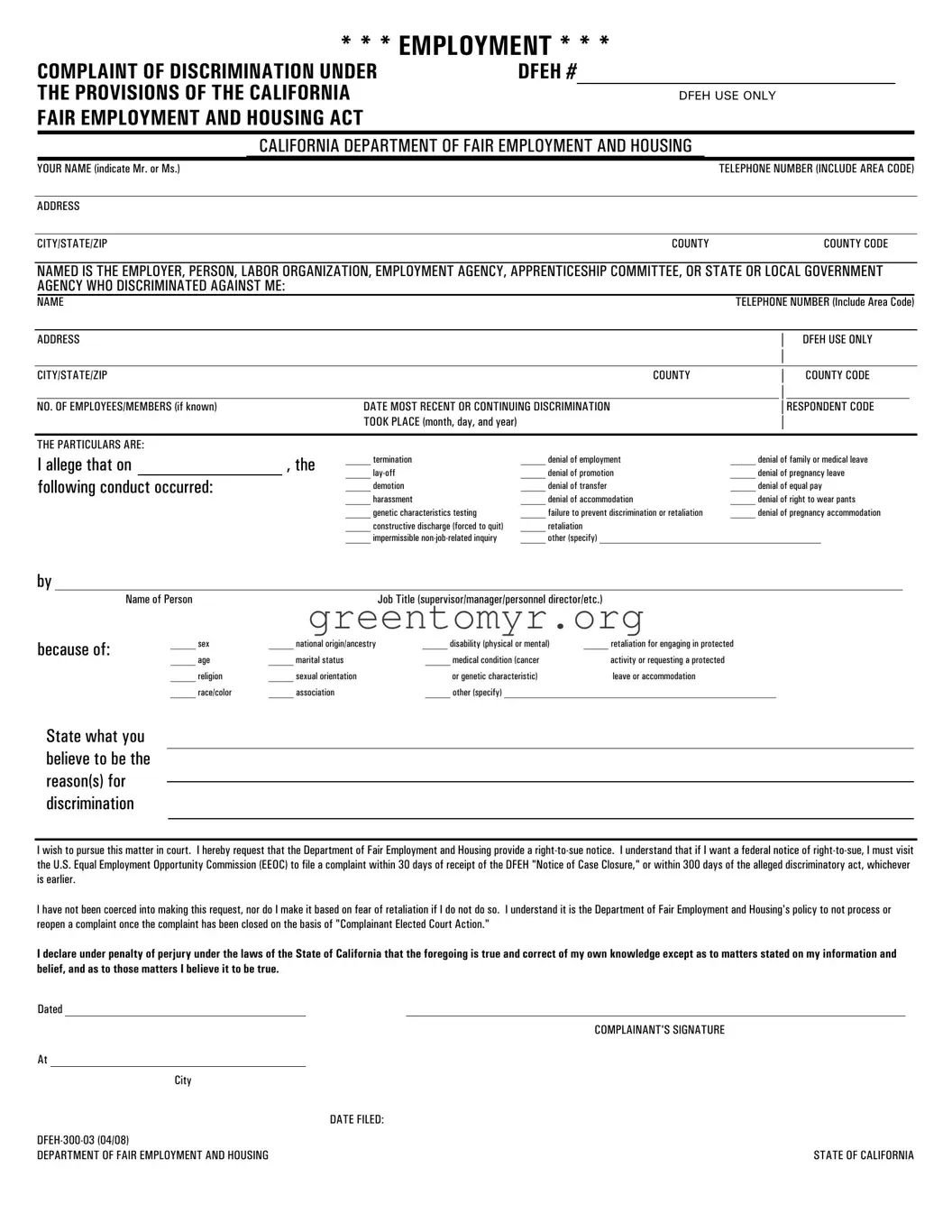
The DFEH 300 03 form serves as a critical tool for individuals seeking to report discrimination under the California Fair Employment and Housing Act. This form is utilized by the California Department of Fair Employment and Housing (DFEH) to collect essential information regarding incidents of discrimination in the workplace. It requires the complainant to provide personal details, including their name, contact information, and address, as well as specifics about the employer or entity that allegedly discriminated against them. Essential questions guide the user to detail the nature of the discrimination, such as termination, harassment, or retaliatory actions, and the characteristics that may have influenced the discriminatory actions, such as gender, race, or disability status. Notably, the form also informs the complainant about their rights to pursue the claim in court, emphasizing the need for timely action and compliance with federal regulations in certain cases. Furthermore, it outlines the requirement for separate complaints if multiple entities are involved, thus ensuring clarity and organization in the reporting process. As a comprehensive document, the DFEH 300 03 form helps individuals navigate the complex path of reporting workplace discrimination effectively.
* * * EMPLOYMENT * * *
COMPLAINT OF DISCRIMINATION UNDER |
DFEH # |
THE PROVISIONS OF THE CALIFORNIA |
|
FAIR EMPLOYMENT AND HOUSING ACT |
|
DFEH USE ONLY
CALIFORNIA DEPARTMENT OF FAIR EMPLOYMENT AND HOUSING
YOUR NAME (indicate Mr. or Ms.) |
|
TELEPHONE NUMBER (INCLUDE AREA CODE) |
|
|
|
ADDRESS |
|
|
|
|
|
CITY/STATE/ZIP |
COUNTY |
COUNTY CODE |
NAMED IS THE EMPLOYER, PERSON, LABOR ORGANIZATION, EMPLOYMENT AGENCY, APPRENTICESHIP COMMITTEE, OR STATE OR LOCAL GOVERNMENT AGENCY WHO DISCRIMINATED AGAINST ME:
NAME |
|
|
TELEPHONE NUMBER (Include Area Code) |
||||
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
│ |
DFEH USE ONLY |
||
|
|
|
|
|
│ |
|
|
CITY/STATE/ZIP |
|
COUNTY |
|
│ |
COUNTY CODE |
||
|
|
|
|
|
│ |
|
|
NO. OF EMPLOYEES/MEMBERS (if known) |
DATE MOST RECENT OR CONTINUING DISCRIMINATION |
|
|
│ |
RESPONDENT CODE |
|
|
|
|
TOOK PLACE (month, day, and year) |
|
|
│ |
|
|
THE PARTICULARS ARE:
I allege that on |
|
, the |
_____ termination |
_____ denial of employment |
_____ denial of family or medical leave |
|
_____ |
_____ denial of promotion |
_____ denial of pregnancy leave |
||||
following conduct occurred: |
|
|||||
|
_____ demotion |
_____ denial of transfer |
_____ denial of equal pay |
|||
|
|
|
||||
|
|
|
_____ harassment |
_____ denial of accommodation |
_____ denial of right to wear pants |
|
|
|
|
_____ genetic characteristics testing |
_____ failure to prevent discrimination or retaliation |
_____ denial of pregnancy accommodation |
|
|
|
|
_____ constructive discharge (forced to quit) |
_____ retaliation |
|
|
|
|
|
_____ impermissible |
_____ other (specify) ____________________________________________ |
||
by
because of:
Name of Person |
|
Job Title (supervisor/manager/personnel director/etc.) |
|
_____ sex |
_____ national origin/ancestry |
_____ disability (physical or mental) |
_____ retaliation for engaging in protected |
_____ age |
_____ marital status |
_____ medical condition (cancer |
activity or requesting a protected |
_____ religion |
_____ sexual orientation |
or genetic characteristic) |
leave or accommodation |
_____ race/color |
_____ association |
_____ other (specify) ______________________________________________________ |
|
State what you believe to be the reason(s) for discrimination
I wish to pursue this matter in court. I hereby request that the Department of Fair Employment and Housing provide a
I have not been coerced into making this request, nor do I make it based on fear of retaliation if I do not do so. I understand it is the Department of Fair Employment and Housing's policy to not process or reopen a complaint once the complaint has been closed on the basis of "Complainant Elected Court Action."
I declare under penalty of perjury under the laws of the State of California that the foregoing is true and correct of my own knowledge except as to matters stated on my information and belief, and as to those matters I believe it to be true.
Dated
At
City
DATE FILED:
DEPARTMENT OF FAIR EMPLOYMENT AND HOUSING
COMPLAINANT'S SIGNATURE
STATE OF CALIFORNIA

DFEH needs a separate signed complaint for each employer, person, labor organization, employment agency, apprenticeship committee, state or local government agency you wish to file against. If you are filing against both a company and an individual(s), please complete separate complaint forms naming the company or an individual in the appropriate area.
Please complete the following so that DFEH can process your complaint and for DFEH for statistical purposes, and return with your signed complaint(s):
YOUR RACE:/ETHNICITY (Check one)
__
__ Asian/Pacific Islander (specify)___________
__ Caucasian
__ Hispanic(specify)____________________
YOUR PRIMARY LANGUAGE (specify)
_______________________________________
YOUR AGE: __ __
IF FILING BECAUSE OF YOUR NATIONAL ORIGIN/ANCESTRY, YOUR NATIONAL ORIGIN/ANCESTRY (specify)
_______________________________________
IF FILING BECAUSE OF DISABILITY,
YOUR DISABILITY:
__ AIDS
__ Blood/Circulation
__ Brain/Nerves/Muscles
__ Digestive/Urinary/Reproduction __ Hearing
__ Heart
__ Limbs (Arms/Legs) __ Mental
__ Sight
__ Speech/Respiratory __ Spinal/Back
IF FILING BECAUSE OF MARITAL STATUS,
YOUR MARITAL STATUS: (Check one)
__ Cohabitation __ Divorced __ Married __ Single
IF FILING BECAUSE OF RELIGION,
YOUR RELIGION: (specify)
____________________________________
IF FILING BECAUSE OF SEX, THE REASON: __ Harassment
__ Orientation __ Pregnancy
__ Denied Right to Wear Pants
__ Other Allegations (List) ________________________
Department of Fair Employment and Housing
State of California
YOUR GENDER: __ Female __ Male
YOUR OCCUPATION: __ Clerical
__ Craft
__ Equipment Operator __ Laborer
__ Manager
__ Paraprofessional __ Professional __ Sales
__ Service __ Supervisor __ Technician
HOW YOU HEARD ABOUT DFEH: __ Attorney
__ Bus/BART Advertisement __ Community Organization __ EEOC
__ EDD __ Friend
__ Human Relations Commission __ Labor Standards Enforcement __ Local Government Agency __ Poster
__ Prior Contact with DFEH __ Radio
__ Telephone Book __ TV
__ DFEH Web Site
DO YOU HAVE AN ATTORNEY WHO HAS AGREED TO REPRESENT YOU ON YOUR EMPLOYMENT DISCRIMINATION CLAIMS IN COURT? IF YOU CHECK “YES”, YOU WILL BE RESPONSIBLE FOR HAVING YOUR ATTORNEY SERVE THIS DFEH COMPLAINT.
__ Yes |
__ No |
PLEASE PROVIDE YOUR ATTORNEY’S NAME, ADDRESS AND PHONE NUMBER:
_______________________________________
_______________________________________
_______________________________________
Your Signature |
Date |
| Fact Name | Description |
|---|---|
| Governing Law | The DFEH 300 03 form is governed by the California Fair Employment and Housing Act (FEHA). |
| Purpose | This form allows individuals to file a complaint of discrimination against their employer or another entity. |
| Eligibility | Any individual who believes they have faced discrimination in employment can use this form. |
| Submission Requirements | DFEH requires a separate form for each entity named in the complaint. |
| Process Flow | Individuals can seek a right-to-sue notice from DFEH after filing a complaint. |
| Filing Deadline | Complaints must be filed within 300 days of the alleged discrimination. |
| Coercion Statement | Signers must declare they are not coerced into requesting the right-to-sue notice. |
| Data Collection | DFEH collects demographic information for statistical purposes. |
| Legal Representation | The form asks if the complainant has an attorney representing them in court. |
Completing the DFEH 300 03 form is an essential step if you believe you've experienced discrimination in your workplace. This form helps the California Department of Fair Employment and Housing (DFEH) understand your situation. Ensure you gather all necessary information and read the instructions carefully to minimize errors.
The DFEH 300 03 form is a complaint form used in California to report instances of employment discrimination. It is governed by the California Fair Employment and Housing Act (FEHA), which aims to protect employees from unfair treatment based on various characteristics, such as race, sex, disability, and age. By completing this form, individuals assert their rights and initiate the process for resolving their discrimination claims.
If you believe you have been discriminated against in your workplace based on characteristics like sex, race, disability, or religion, you may need to file a complaint. Signs of potential discrimination include unfair treatment, harassment, or denial of rights related to your employment. If you are unsure, consulting with a legal professional can provide clarity on your situation.
The form requires detailed information, including:
Completing this information accurately is crucial for the processing of your complaint.
Yes, if you have multiple employers or individuals involved in your claim, you must complete separate complaint forms for each one. This ensures that each case is treated individually and properly investigated.
After submitting the form, the DFEH will review your complaint. They may initiate an investigation to gather more information about your claim. You will be notified of the outcome, and if the DFEH closes your case, you can request a right-to-sue notice, allowing you to pursue the matter in court if you wish.
A right-to-sue notice is a legal document issued by the DFEH confirming that they will not take further action on your complaint. This notice enables you to file a lawsuit in civil court regarding your discrimination claim. Keep in mind, if you’re considering going this route, specific deadlines apply for filing, so it is essential to act promptly.
Typically, you have one year from the date of the discriminatory act to file a complaint with the DFEH. However, if you decide to pursue a federal claim through the Equal Employment Opportunity Commission (EEOC), much shorter deadlines may apply. It is crucial to be mindful of these timelines to ensure your claim is accepted.
No, you do not need an attorney to file a DFEH complaint. Many individuals successfully navigate the process on their own. However, having legal representation can provide additional support, especially if your case escalates to court. If your claim involves complex issues, consulting an attorney might be beneficial.
It is understandable to worry about retaliation after filing a complaint. California law protects employees from retaliation for asserting their rights regarding discrimination. If you experience any retaliatory actions, document them and report them immediately, as these actions could warrant further legal action.
A common mistake people make when filling out the DFEH 300 03 form is not providing complete contact information. This includes failing to list a valid telephone number or address. Without accurate contact details, DFEH may have difficulty reaching you for updates or further information.
Another frequent error is neglecting to specify the correct employer or entity involved in the discrimination claim. It's essential to include all relevant names, such as the employer, individual supervisors, or associated organizations. A vague or incomplete naming can delay the processing of your complaint.
People often forget to include the date when the most recent discrimination occurred. Noting this date is crucial because it impacts the timeline for your complaint. Without a specific date, it can complicate matters down the road.
A significant oversight is not detailing the exact nature of the discrimination. Simply checking boxes on the form without elaborating on the circumstances may not provide enough information. Clearly stating your allegations can help the DFEH better understand your situation and take appropriate action.
When listing the reasons for discrimination, individuals sometimes miss the chance to explain their claims thoroughly. Providing specific examples or instances can strengthen your complaint and give context to the situation.
Another common mistake is not signing or dating the form. An unsigned or undated form may be considered incomplete. Make sure you provide your signature along with the date to ensure that your complaint is valid.
Some individuals incorrectly assume they only need one form, even when filing against multiple respondents. It’s crucial to submit separate forms for each employer or individual to avoid delays and confusion in processing.
Finally, people sometimes skip the section that asks about prior contact with attorneys or legal representation. If you have an attorney, you need to provide their information. This helps DFEH manage communication effectively and ensures your rights are protected.
The DFEH 300 03 form serves as a vital document when filing a discrimination complaint under the California Fair Employment and Housing Act. In addition to this form, several other documents may be required to support your case. Each plays a role in ensuring that your complaint is processed correctly and efficiently.
When preparing your complaint, it is essential to ensure all necessary forms and supporting documentation are included. This completeness helps facilitate a smoother process in seeking resolution for employment discrimination claims.
The DFEH 300 03 form is a document designed for individuals who wish to file a complaint of discrimination under the California Fair Employment and Housing Act. However, there are several other legal forms that serve similar purposes. Here’s a rundown of nine documents that are comparable to the DFEH 300 03 form:
Each of these documents serves essential functions and helps individuals navigate their rights in employment situations. It’s comforting to know that whatever the specific circumstances may be, there are pathways and forms available to address grievances and seek justice.
Dos:
Don'ts:
There are numerous misconceptions about the DFEH 300 03 form. Addressing these might help clarify the process for those seeking to file a complaint. Below are ten common misunderstandings regarding this important document:
It is essential to understand these clarifications when navigating the complaint process with the DFEH. Knowledge can empower you to take the right actions moving forward.
Here are key takeaways about filling out and using the DFEH 300 03 form: