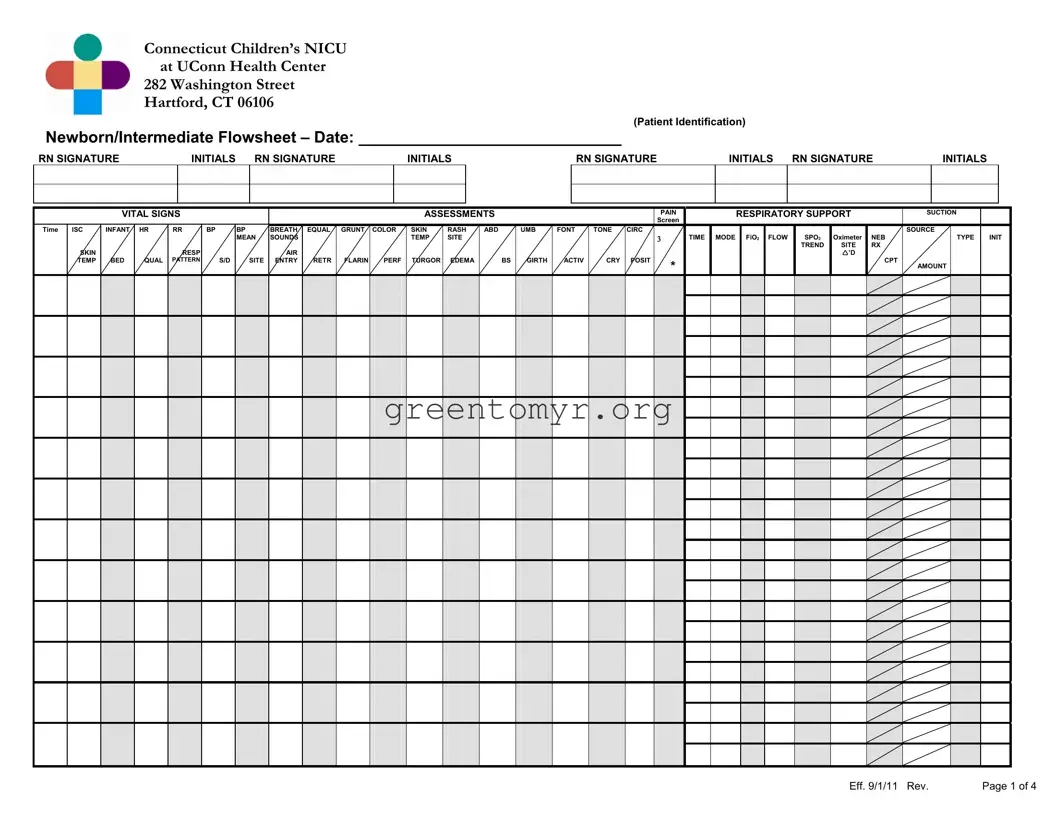
The ICU Flowsheet form is an essential tool for monitoring the health and development of newborns in the intensive care setting. Captured on this form are critical details that healthcare providers rely on daily. It encompasses vital signs, including heart rate, respiratory rate, and temperature, recorded meticulously by nurses. The form not only charts these numerical data points but also highlights assessments on pain levels, respiratory support, and skin conditions. Importantly, the Flowsheet is designed to document various interventions and treatments administered, such as phototherapy and IV therapy, ensuring a comprehensive record of the infant's care. Aspects like family education and communication also find space here, emphasizing the collaboration between healthcare professionals and families. Additionally, safety protocols regarding alarms for heart rate and respiratory concerns are included, adding another layer of vigilance. Aligned with the standards of care and discharge planning, this tightly structured and detailed flowsheet transforms raw data into actionable insights, ultimately guiding the infant's recovery and overall well-being.
Connecticut Children’s NICU
at UConn Health Center
282 Washington Street
Hartford, CT 06106
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Patient Identification) |
|
|
|
|
|
|
|
|
|
|||||||
Newborn/Intermediate Flowsheet – Date: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
RN SIGNATURE |
|
|
INITIALS |
|
RN SIGNATURE |
|
|
|
|
INITIALS |
|
|
|
RN SIGNATURE |
|
|
|
INITIALS |
RN SIGNATURE |
|
INITIALS |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
VITAL SIGNS |
|
|
|
|
|
|
|
|
|
ASSESSMENTS |
|
|
|
|
|
PAIN |
|
|
RESPIRATORY SUPPORT |
|
SUCTION |
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Screen |
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time |
ISC |
INFANT |
HR |
RR |
BP |
BP |
BREATH |
EQUAL |
GRUNT |
COLOR |
SKIN |
RASH |
ABD |
UMB |
FONT |
TONE |
CIRC |
|
|
|
|
|
|
|
|
|
|
|
SOURCE |
|
|
||||||||
|
|
|
|
|
|
|
MEAN |
SOUNDS |
|
|
|
|
|
TEMP |
SITE |
|
|
|
|
|
|
|
TIME |
MODE |
FiO2 |
FLOW |
|
SPO2 |
Oximeter |
NEB |
|
|
TYPE |
INIT |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TREND |
SITE |
RX |
|
|
|
|
|
|
SKIN |
|
|
|
RESP |
|
|
|
AIR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
’D |
|
|
|
|
|
|
|
TEMP |
BED |
QUAL |
PATTERN |
S/D |
SITE |
ENTRY |
RETR |
FLARIN |
PERF |
TURGOR |
EDEMA |
BS |
GIRTH |
ACTIV |
CRY |
POSIT |
* |
|
|
|
|
|
|
|
|
|
CPT |
AMOUNT |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Eff. 9/1/11 Rev. |
Page 1 of 4 |
Connecticut Children’s NICU
at UConn Health Center
282 Washington Street
Hartford, CT 06106
(Patient Identification)
Newborn/Intermediate Flowsheet – Date:
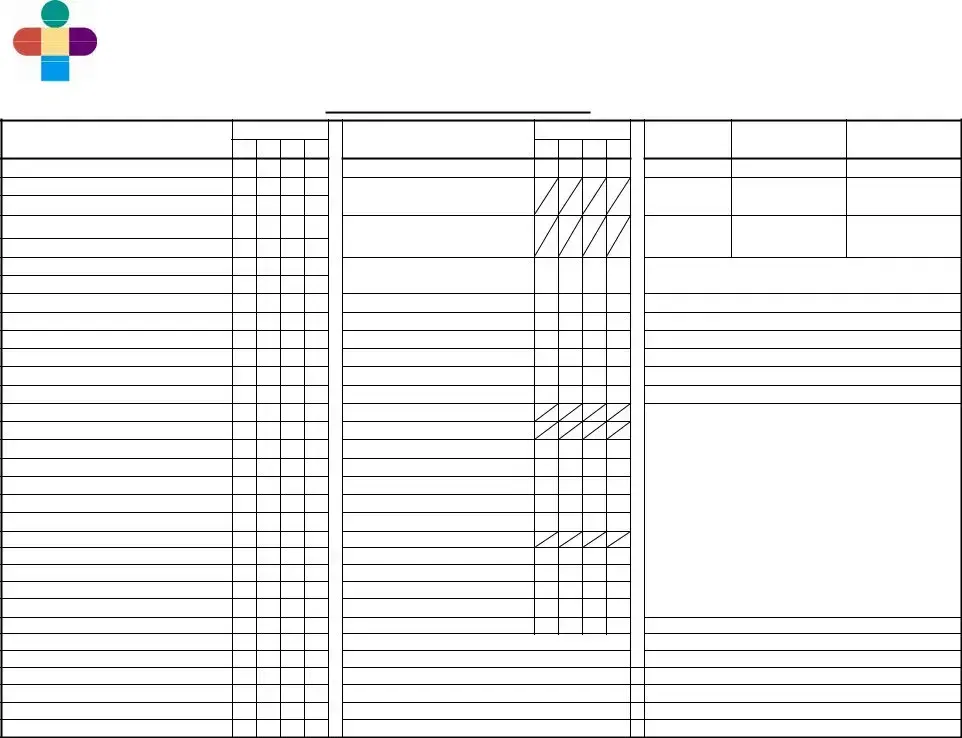
Standards of Care |
SHIFT |
Care of the Infant with:
Admission to the Newborn Nursery
Apnea/ Bradycardia /Periodic Breathing
Breastfeeding/Breast Pumping
Bronchodilators
Cardiorespiratory Monitor
Central Lines
Circumcision
Developmental Assessment and Care
Discharge Planning: Neonatal
Feeding: NG/OG/Continuous/Intermittent
GE Reflux
Grieving
Hospitalized Infant: Care of the Family
IV Therapy
Kangaroo Care
Pain Screening and Assessment
Phototherapy/Biliblanket
Pulse Oximetry
Skin Care: Neonatal
Steroids
Supplemental Oxygen
Thermoregulation
Well Newborn
Other:
PATIENT AND FAMILY TEACHING RECORDS:
Family Education of the hospitalized Infant
BPD
Others:
SHIFT
SAFETY:
ALARMS:
HR: HIGH / LOW
RR: HIGH/Apnea > 20 sec.
Pulse Oximetry: Low
Security Sensor On:
EQUIPMENT:
Resuscicard
Bag/Mask & O2 Flow
Suction
ID & Blood Bracelet
Evacuation Pack & ID
PHOTOTHERAPY:
Photo Tx Intensity
Eye Patches
Serum Bili Level
HYGIENE:
Bath/Linens
Cord Care
Circ. Care
Nares Care
Mouth Care
PARENT COMMUNICATION:
WEIGHT: |
KG |
LB |
Birth Weight:
Yesterday:
Today:
Wt change:
Length:OFC:
Corrected Gestational Age:
Mom’s Room #
Care Level:
Physician:
BLOOD GAS RESULTS
Time |
Site |
pH |
pCO2 |
pO2 |
BE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAB TESTS/RESULTS
Time |
Site |
Gluc |
HCT |
TESTS AND RESULTS |
|
Meter |
|||||
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STOOL/URINE RESULTS
COMMENTS:
Eff. 9/1/11 Rev. |
Page 2 of 4 |

Connecticut Children’s NICU
at UConn Health Center
282 Washington Street
Hartford, CT 06106
(Patient Identification)
Newborn/Intermediate Flowsheet – Date:
GENERAL
R – Right
L – Left
- Done
-- Absent
+ - Present - Increased - Decreased
‡- Asymmetrical = - Equal
- Changed
BED
I – Isolette
OC – Open Crib
OW – Open Warmer
HR QUALITY
R – Regular
I – Irregular
M – Murmur
RESP. PATTERN
R – Regular
IR – Irregular
S – Shallow
PB – Periodic
Breathing
BP SITE
LA – Left Arm RA – Right Arm
LL– Left Calf RL – Right Calf LT – Left Thigh RT – Right Thigh
BREATH SOUNDS
Cr – Crackles
C – Clear
CO – Coarse
W – Wheeze
S – Stridor
AIR ENTRY
G – Good
L – Limited
T – Tight
EQUALITY
++- Bilaterally RorL - Diminished - Diminished
bilaterally
RETRACTIONS
M – Minimal
MO – Moderate
S – Severe
GRUNTING |
UMBILICAL |
POSITION/MISC |
STOOL COLOR |
ORAL(PO) FEEDING DESCRIPTION |
||
A – Audible w/naked |
CORD |
P - Prone |
M – Meconium |
|
|
|
|
ear |
O - Off |
S – Supine |
Y – Yellow |
BEHAVIOR BEFORE FEEDING |
|
S – Stethescope only |
D - Dry |
R - Rt. Side Down |
G – Green |
1 |
Infant awakens on own signaling |
|
Int - Intermittent |
W - Wet |
L - Lt. Side Down |
B – Brown |
|
hunger with crying or fussing; shows |
|
|
|
Cl - Clamped |
HOB - Head of Bed Up |
FB – FRANK BLOOD |
|
hunger cues (rooting, sucking, |
COLOR |
DG - Drainage |
HOB - Head of Bed |
|
|
searching, hand to mouth). |
|
P - Pink |
R – Erythema |
Down |
CONSISTENCY |
2 Infant awakens on own, may remain |
||
W – Pale |
confined to |
IS – Infant Seat |
S – Soft |
|
quietly alert, drowsy or begin fussing or |
|
D – Dusky |
stump |
SW – Swaddled |
W - Watery |
|
moving, may show some hunger cues |
|
C – Cyanotic |
Rt – Erythema |
SG – Swing |
P – Pasty |
|
(rooting, sucking, searching, hand to |
|
J – Jaundiced |
extended to |
H – Held |
SD – Seedy |
|
mouth). |
|
PL – Plethoric |
abdominal |
|
Mu – Mucous |
3 |
Infant awakens with |
|
M – Mottled |
wall |
OXYGEN MODE |
|
|
begins to show hunger cues (rooting, |
|
A |
|
I – Isolette |
ENTERAL FEEDS |
|
sucking, searching, show hand to |
|
|
|
FONTANELLE |
H – Hood |
MODE |
|
mouth, fussing). |
PERFUSION |
S – Soft, Flat |
NC – Nasal Cannula |
Po – Nipple |
4 |
Infant awakens with |
|
N – CRT < 3 sec. |
F – Full |
MT – Mist tent |
BF – Breastfeeding |
|
appears quietly awake or somewhat |
|
A – CRT > 3 sec. |
T – Tense |
TC – Trach Collar |
CNG – Continuous |
|
drowsy with limited hunger cues |
|
|
|
B – Bulging |
CPT |
Nasogastric |
|
(rooting, sucking, searching, hand to |
SKIN TEMP |
D – Depressed |
P – Percussion |
NG/OG – Gavage |
|
mouth). |
|
W – Warm |
|
V – Vibration |
|
5 |
Infant remains asleep or drowsy. |
|
C – Cool |
ACTIVITY |
|
IV SITE CHECK |
6 |
Infant appears to have limited |
|
H – Hot |
++ - Active, Alert |
SUCTION SOURCE |
W – Warm |
|
physiological stamina required to |
|
D - Diaphoretic |
+ - Active to stim |
O – Oral |
C – Cool |
|
sustain control and endurance for |
|
|
|
L - Lethargic |
N- Nares |
E – Edematous |
|
feeding attempt. |
TURGOR |
S - Sleeping |
|
R – Erythematous |
BEHAVIOR DURING BOTTLE FEEDING |
||
G – Good |
NC - Non- |
SUCTION AMOUNT |
N – |
1 |
Energetic with steady, coordinated |
|
F – Fair |
consolable |
S – Small |
|
|||
P – Poor |
Q – Quiet |
Mo – Moderate |
|
to no in resp. effort or color; easily |
||
C - Crepitus |
|
L – Large |
Bl – Blanched |
|
maintains tone, posture, remains calm |
|
|
|
TONE |
|
|
|
and completes feeding. |
RASH SITE |
N - Normal |
TYPE |
IV LOCATION |
2 |
Initially energetic with steady, |
|
PA – Perianal |
- Hypertonic |
Th – Thin |
RAc – Right Antecubital |
|
coordinated |
|
PN – Perineal |
- Hypotonic |
Tk – Thick |
LAc – Left Antecubital |
|
challenges |
|
G – Generalized |
J - Jittery |
C – Clear |
RF – Right Foot |
|
coordination, in resp. effort, color, |
|
T – Trunk |
C – Clonus |
W – White |
LF – Left Foot |
|
tone, posture or state) with support, is |
|
|
|
|
Y – Yellow |
RH – Right Hand |
|
able to complete feeding. |
EDEMA |
CRY |
G – Green |
LH – Left Hand |
3 Initially slow to start or passive; has |
||
G – Generalized |
L - Lusty, |
BRB – Bright Red Blood |
RW – Right Wrist |
|
challenges (with |
|
Ex – Hands and Feet |
Vigorous |
P – Plugs |
LW – Left Wrist |
|
coordination, resp. effort, color, tone, |
|
PO – Periorbital |
W - Weak |
Br – Brown |
RAk – Right Ankle |
|
posture or state); needs support |
|
|
|
Hi - |
|
LAk – Left Ankle |
|
throughout and may or may not |
ABDOMINAL |
A - Appropriate |
ASPIRATE TYPE |
S – Scalp |
|
complete feeding. |
|
S – Soft |
for age |
M – Mucous |
B – Broviac |
4 |
Initially energetic or slow to start; |
|
ND – |
F – Formula |
PQ – |
|
becomes disorganized; shows |
||
Ts – Tense |
Q - Quiet |
B – Bilious |
|
|
instability (in |
|
Tn – Tender |
|
FB – Frank Blood |
BLOOD GAS SITE |
|
coordination, resp. effort, color, tone, |
|
DC – Discolored |
PAIN SCREEN |
CG – Coffee Ground |
HS – Heel Stick |
|
posture or state); is unable to complete |
|
D – Distended |
pain screen |
A – Air |
VS – Venous Stick |
|
feeding. |
|
F – Full |
|
FS – Finger Stick |
5 |
(*) Concerning feeding behaviors or |
||
|
|
“triggers” for pain |
DISPOSITION |
Art – Arterial Stick |
|
oral motor patterns; may appear |
BOWEL SOUNDS |
*Refer to pain |
A – Aspirate |
|
|
disinterested or upset with feeding |
|
- |
- Absent |
assessment |
D- Discarded |
CIRC |
|
attempts or may awaken but is unable |
+ |
- Present, Active |
scale |
R- Ref |
CL – Clean |
|
to coordinate |
- Decreased |
|
|
DG – Drainage |
|
|
|
- Hyperactive |
|
|
BL - Bleeding |
|
|
|
BEHAVIOR DURING BREASTFEEDING
1Latches on without difficulty with strong, steady and rhythmic sucks; briefly pauses and readily resumes sucking; frequent,
coordinated suck- swallowing heard
2Latches on without difficulty with strong, steady and rhythmic sucks; briefly pauses
and resumes sucking without help; some swallowing heard.
3 Latches on with minimum difficulty; sucks are short and quick without steady rhythm; pauses and needs help to resume sucking; occasional swallowing heard.
4Roots or licks; latches on with difficulty; briefly maintains latchon or does not suck;
no swallowing heard.
5 Roots or licks; unable to latch on for breastfeeding attempt.
6No effort (sleepy, lacks energy, has no interest, cries, squirms, or pushes away) despite much assistance, unable to successfully attempt breastfeeding.
RESPONSE TO FEEDING
1Appears satiated and comfortable; becomes relaxed, quietly interactive or sleepy without
physiologic changes.
2Becomes tired and fatigued from feeding; has minimal in HR, resp, color or tone.
3Exhausted or taxed by feeding; has changes in resp, color, loss of tone or other
physiologic signs (hiccups, grunts/sounds, cough/choke, head bobbing, O2 sats)
resulting from efforts to feed.
4Has difficulty settling; appears uncomfortable following feeding (shifting within position, straining, spitting, fussiness and/or increased respiratory effort).
SUPPORTS
OB - Occasional Breaks/Pauses
FB - Frequent Breaks/Pauses
PH - Pacing Help
BU - Frequent Burps
FA
SP - Sidelying Position
OP - Other Position
CS - Chin/Cheek Support
OX - Oxygen
EN - Environment
Other - Specify
TYPE OF NIPPLE |
|
|
Y - Yellow |
SF- Slow Flow |
|
R - Red |
P - Playtex |
|
N - Nuk |
H - Haeberman |
|
G – Gerber Premie |
SL=Slit |
|
Eff. 9/1/11 Rev. |
Page 3 of 4 |
|
Connecticut Children’s NICU
at UConn Health Center
282 Washington Street
Hartford, CT 06106
(Patient Identification)
Newborn/Intermediate Flowsheet – Date:
|
|
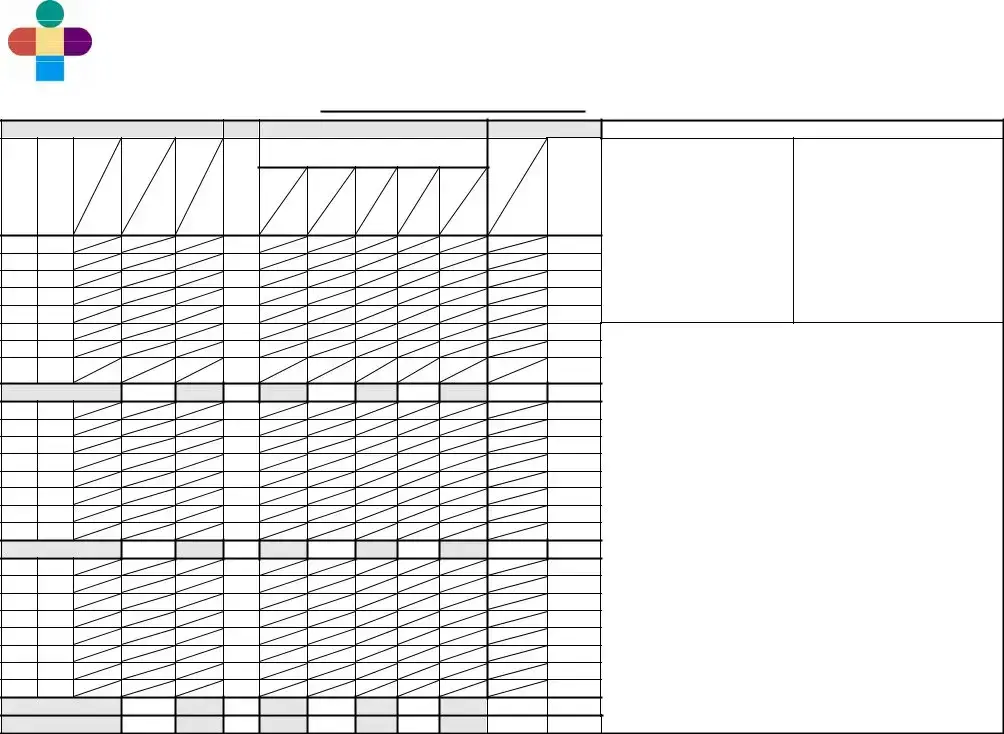
ENTERAL INTAKE |
|
|
|
PARENTERAL INTAKE |
|
|
OUTPUT |
||||
|
|
|
|
|
|
|
Solution: |
|
|
|
|
|
|
|
|
MODE |
TOTAL |
|
|
E |
|
|
|
|
|
URINE |
STOOL |
T |
F |
|
|
|
|
M |
|
|
|
|
|
|
AMT |
I |
O |
|
|
ASP |
|
E |
Dext% |
Total |
IL |
Total |
Site |
|
COLOR |
M |
R |
|
|
|
S |
|
CONSIS |
||||||
|
|
|
|
|
|
|
|
|
|||||
|
|
AMT |
|
|
|
|
|
|
|
||||
E |
M |
|
|
|
I |
|
|
|
|
|
|
|
|
|
|
|
Type |
|
|
|
|
|
|
|
|||
|
U |
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
L |
RATE |
Hourly |
|
|
|
Rate |
|
|
|
|
|
|
|
A |
|
Bolus |
|
|
|
|
|
|
|
URINE |
|
|
|
|
|
|
|
|
Hourly |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
W/STOOL |
|
|
|
|
|
|
|
|
|
|
|
Rate |
Hourly |
Location |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
FORMULA
SUPPLEMENTS
FORMULA TYPE/CALORIE
#1__________________________
#2__________________________
#3__________________________
ORAL (PO) FEEDING DESCRIPTION * See Codes
T |
Behavior |
Attempt |
Behavior |
Response |
|
|
Type |
||
I |
Before |
PO |
During |
to |
Duration |
Supports |
of |
||
M |
|||||||||
|
|
Feeding |
|
|
|
|
|||
E |
Feeding |
Y/N |
Feeding |
|
|
Nipple |
|||
|
|
|
|
||||||
|
|
|
BOTTLE BREAST |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMMENTS:_______________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
Eff. 9/1/11 Rev. |
Page 4 of 4 |
| Fact Name | Description |
|---|---|
| Facility Name | Connecticut Children’s NICU at UConn Health Center in Hartford, CT, is the facility where the flowsheet is used. |
| Purpose | This flowsheet is designed to document patient care for newborns and infants in the NICU. |
| Patient Identification | The form includes a section for patient identification to ensure accurate tracking of each infant's care. |
| Vital Signs Recording | Vital signs including heart rate, respiratory rate, and blood pressure are required to be documented regularly on the sheet. |
| Assessment Areas | Multiple assessment categories, including pain and respiratory support, are included to monitor the infant's condition comprehensively. |
| Shift Care Protocol | This flowsheet adheres to specific standards of care for various conditions like apnea, bradycardia, and breastfeeding. |
| Parental Communication | There is a section dedicated to documenting parent communication, ensuring family involvement in care. |
| Legal Compliance | This form is compliant with Connecticut state regulations for pediatric care and documentation standards. |
| Revision Date | The latest revision date for the form is September 1, 2011, indicating when updates were last made. |
| Documentation Importance | Accurate and timely documentation on this flowsheet is crucial for effective care management and review. |
Filling out the Icu Flowsheet form is an important task for ensuring the proper monitoring of the newborn's health. This document collects vital information about the infant’s condition and treatment, allowing for effective care management. It is essential to complete each section accurately to provide a clear and comprehensive record.
Review the completed form to ensure that all information is accurate and clear. This documentation will guide ongoing care and treatment decisions for the newborn, ensuring they receive the attention they require.
The ICU Flowsheet form is designed to provide a systematic way to record the clinical data of infants in a Neonatal Intensive Care Unit (NICU). It tracks vital signs, assessments, medication administration, and other essential care details. This helps healthcare providers monitor the infant's condition, make informed decisions, and ensure continuity of care.
The flowsheet captures a variety of critical information, including:
The registered nurse (RN) is primarily responsible for completing the ICU Flowsheet. RNs continuously monitor the infant's condition, document care activities, and ensure that all required information is accurately recorded. It is a collaborative effort, however, as other healthcare professionals may also contribute specific data.
The ICU Flowsheet should be updated whenever there is a significant change in the infant's condition or after each assessment. Typically, it is updated at the start of each shift and as needed throughout the day to ensure all information is current and accurate.
Key vital signs monitored include:
Monitoring these parameters is essential for providing immediate care and interventions as needed.
The flowsheet serves as a tool for communicating relevant information to families. It documents the educational efforts provided to the family about the infant's condition, care plan, and feeding practices. By reviewing the flowsheet, families can better understand their infant's care and progress.
If incorrect information is found, it is crucial to correct it as soon as possible. The RN should draw a single line through the error, write the correct information, and initial the change. This ensures that everyone reviewing the flowsheet can easily understand what was corrected without obscuring the original information.
The flowsheet plays a vital role in discharge planning by documenting necessary care milestones that need to be achieved before discharge. It includes notes on patient readiness, family education, and follow-up care instructions. This thorough documentation helps ensure a safe transition home.
Completing the Icu Flowsheet form is a crucial step in ensuring the best care for patients in the NICU. However, there are common mistakes that can compromise the accuracy and completeness of this important document. Awareness of these pitfalls can help nursing staff and caregivers avoid errors.
One common mistake is failing to include patient identification details. Each flowsheet must begin with the newborn's identification to ensure that the data corresponds correctly to the right patient. Without proper identification, any information recorded can lead to significant errors in treatment and care.
Another frequent error involves not documenting all required vital signs. The flowsheet must contain clear readings for heart rate, respiration rate, blood pressure, and temperature. Skipping any of these can create gaps in a patient's health record, making it difficult for medical personnel to assess their condition accurately.
Inconsistent or unclear documentation can also be a significant mistake. Abbreviations and shorthand can vary greatly between nurses, leading to confusion about what specific entries mean. Ensuring clarity is vital for other team members who will reference the flowsheet later. Writing complete descriptions, when necessary, helps maintain clear communication.
Avoiding the entry of subjective assessments is insightfully important. Objective data should always take precedence when filling out the flowsheet. For example, noting evident physical signs or behaviors is better for tracking a newborn’s condition than stating how the baby "seems.” Relying on observations rather than interpretations improves accuracy.
People often forget to make necessary updates throughout the shift. This includes recording changes in vital signs or behaviors as they occur. They might only complete entries at the beginning or end of their shift, missing critical data that can affect ongoing treatment.
Lastly, there can be failure to communicate with other team members about the entries made. Collaboration is key in the NICU, and discussing important observations or changes ensures that staff members are on the same page regarding the newborn's needs. Regular communication can help prevent misunderstandings or oversights when it comes to patient care.
By being mindful of these common mistakes, medical staff can improve the accuracy and efficiency of completing the Icu Flowsheet form, ultimately ensuring better outcomes for the patients under their care.
The following list details other essential forms and documents commonly used alongside the ICU Flowsheet. These documents support the evaluation, treatment, and documentation of care for patients in a neonatal intensive care unit (NICU) setting. Each form plays a specific role in ensuring thorough patient care, facilitating communication among healthcare providers, and maintaining comprehensive medical records.
These forms collectively enhance patient care quality and safety within the NICU environment. By utilizing these documents, healthcare teams can address all aspects of a patient’s treatment and ensure that records are accurate and up to date.
Patient Care Flowsheet: Similar to the ICU Flowsheet, the Patient Care Flowsheet offers a structured way to document patient assessments, interventions, and outcomes during their hospital stay. Both forms capture vital and clinical information, making it easy to track changes over time.
Nursing Assessment Form: This document focuses on the comprehensive evaluation of a patient's physical, psychological, and social needs. Like the ICU Flowsheet, it includes sections for vital signs and various assessments, enabling nurses to understand the patient's condition in detail.
Medication Administration Record (MAR): The MAR details medications given to a patient, including dosages and times. Similar to the ICU Flowsheet, it serves as an important tracking tool, ensuring that medication regimens are followed accurately.
Vital Signs Record: This document is specifically designed to log a patient's vital signs, such as heart rate, blood pressure, and temperature. It shares a common purpose with the ICU Flowsheet in terms of monitoring and alerting healthcare providers to any significant changes in a patient's status.
Clinical Pathway Document: This pathway outlines the expected course of treatment for specific diagnoses. Both the Clinical Pathway Document and the ICU Flowsheet help guide care by detailing assessments and interventions tailored to the patient's needs.
Progress Notes: These notes provide updates on a patient’s condition and treatment. Like the ICU Flowsheet, they summarize observations and care provided during a specific shift, ensuring continuity of care among healthcare professionals.
Discharge Summary: This document encapsulates the patient’s hospital stay and the care received, along with plans for follow-up. It serves a similar purpose to the ICU Flowsheet in terms of highlighting significant health information and ensuring that the necessary information is communicated to other health providers.
Care Plan: A Care Plan details the various aspects of a patient's treatment and goals. It is similar to the ICU Flowsheet in that both are essential for documenting care strategies and assessing the patient's progress toward their health outcomes.
When filling out the Icu Flowsheet form, attention to detail is crucial. Here are some dos and don'ts to guide you through the process.
Misconceptions about the ICU Flowsheet form can lead to confusion and mismanagement in critical care environments. Here are eight common misunderstandings:
Correcting these misconceptions can lead to improved patient outcomes and more efficient care in the ICU setting.
Using the ICU Flowsheet form effectively is vital for tracking the health and care of newborns in the neonatal intensive care unit (NICU). Here are some key takeaways to consider: