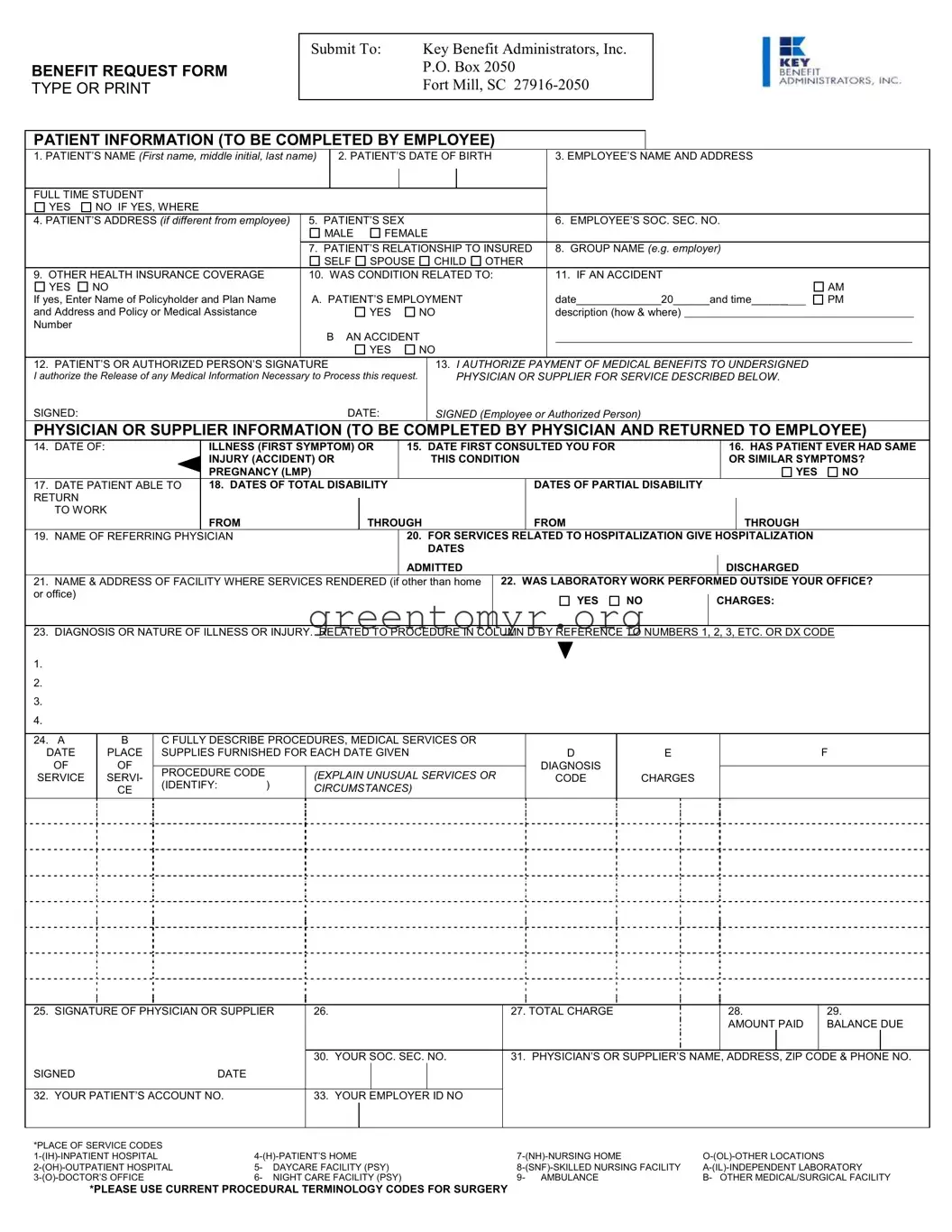
The Key Benefit Request form serves as an essential tool for employees seeking medical benefits on behalf of themselves or their dependents. This form is structured to collect vital patient information, including names, birthdates, and relationships to the insured, ensuring that the claims process is as thorough as possible. Employees must input their social security numbers and indicate any other health insurance coverage that may affect the claim. Additionally, the form prompts questions regarding the nature of the medical condition, including whether it was linked to an accident, alongside necessary signatures for authorizing the release of medical information. Physicians also play a crucial role in this process; they must complete their section by providing dates of illness, diagnosis codes, and details about the medical services rendered. The detailed breakdown of charges and services, including any relevant hospitalization information, is vital for accurate processing. Not only does this form streamline communication between patients, healthcare providers, and insurers, but it also promotes clear documentation that facilitates the approval of medical benefits. Recognizing the importance of careful completion, individuals must ensure that all required fields are filled out accurately to avoid delays in processing their claims.
BENEFIT REQUEST FORM TYPE OR PRINT
Submit To: |
Key Benefit Administrators, Inc. |
|
P.O. Box 2050 |
|
Fort Mill, SC |
|
|
PATIENT INFORMATION (TO BE COMPLETED BY EMPLOYEE)
1. PATIENT’S NAME (First name, middle initial, last name) |
|
2. PATIENT’S DATE OF BIRTH |
|
3. EMPLOYEE’S NAME AND ADDRESS |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FULL TIME STUDENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO IF YES, WHERE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. PATIENT’S ADDRESS (if different from employee) |
5. PATIENT’S SEX |
|
|
|
6. EMPLOYEE’S SOC. SEC. NO. |
|
|
|
||||||||
|
|
MALE |
FEMALE |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
7. PATIENT’S RELATIONSHIP TO INSURED |
|
8. GROUP NAME (e.g. employer) |
|
|
|
|||||||||
|
|
SELF |
SPOUSE |
CHILD OTHER |
|
|
|
|
|
|
|
|
||||
9. OTHER HEALTH INSURANCE COVERAGE |
10. WAS CONDITION RELATED TO: |
|
11. IF AN ACCIDENT |
|
|
|
||||||||||
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
AM |
||
If yes, Enter Name of Policyholder and Plan Name |
A. PATIENT’S EMPLOYMENT |
|
date______________20______and time______ |
PM |
||||||||||||
and Address and Policy or Medical Assistance |
|
|
|
YES |
NO |
|
description (how & where) |
|
|
|
|
|
||||
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
AN ACCIDENT |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
YES |
NO |
|
|
|
|
|
|
|
|
||
12. PATIENT’S OR AUTHORIZED PERSON’S SIGNATURE |
|
|
|
13. I AUTHORIZE PAYMENT OF MEDICAL BENEFITS TO UNDERSIGNED |
|
|
|
|||||||||
I authorize the Release of any Medical Information Necessary to Process this request. |
|
PHYSICIAN OR SUPPLIER FOR SERVICE DESCRIBED BELOW. |
|
|
|
|||||||||||
SIGNED:DATE:
SIGNED (Employee or Authorized Person)
PHYSICIAN OR SUPPLIER INFORMATION (TO BE COMPLETED BY PHYSICIAN AND RETURNED TO EMPLOYEE)
14. |
DATE OF: |
ILLNESS (FIRST SYMPTOM) OR |
15. DATE FIRST CONSULTED YOU FOR |
|
|
|
16. HAS PATIENT EVER HAD SAME |
|||||
|
|
INJURY (ACCIDENT) OR |
|
THIS CONDITION |
|
|
|
OR SIMILAR SYMPTOMS? |
||||
|
|
PREGNANCY (LMP) |
|
|
|
|
|
|
|
|
YES |
NO |
17. |
DATE PATIENT ABLE TO |
18. DATES OF TOTAL DISABILITY |
|
|
DATES OF PARTIAL DISABILITY |
|
|
|
|
|
||
RETURN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
TO WORK |
|
|
|
|
|
|
|
|
|
|
|
|
|
FROM |
THROUGH |
|
FROM |
|
|
|
|
THROUGH |
|
|
19. |
NAME OF REFERRING PHYSICIAN |
|
20. FOR SERVICES RELATED TO HOSPITALIZATION GIVE HOSPITALIZATION |
|
||||||||
|
|
|
|
DATES |
|
|
|
|
|
|
|
|
|
|
|
|
ADMITTED |
|
|
|
|
|
DISCHARGED |
|
|
21. |
NAME & ADDRESS OF FACILITY WHERE SERVICES RENDERED (if other than home |
22. WAS LABORATORY WORK PERFORMED OUTSIDE YOUR OFFICE? |
||||||||||
or office) |
|
|
|
|
YES |
NO |
|
CHARGES: |
|
|||
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
23.DIAGNOSIS OR NATURE OF ILLNESS OR INJURY. RELATED TO PROCEDURE IN COLUMN D BY REFERENCE TO NUMBERS 1, 2, 3, ETC. OR DX CODE
1.
2.
3.
4.
24. A |
B |
C FULLY DESCRIBE PROCEDURES, MEDICAL SERVICES OR |
|
|
|
||
DATE |
PLACE |
SUPPLIES FURNISHED FOR EACH DATE GIVEN |
D |
E |
F |
||
OF |
OF |
|
|
|
DIAGNOSIS |
|
|
PROCEDURE CODE |
|
(EXPLAIN UNUSUAL SERVICES OR |
|
|
|||
SERVICE |
SERVI- |
|
CODE |
CHARGES |
|
||
(IDENTIFY: |
) |
|
|||||
|
CE |
CIRCUMSTANCES) |
|
|
|
||
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
25. SIGNATURE OF PHYSICIAN OR SUPPLIER |
26. |
|
|
|
|
27. TOTAL CHARGE |
|
28. |
|
|
29. |
|
||
|
|
|
|
|
|
|
|
|
|
AMOUNT PAID |
|
BALANCE DUE |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
30. |
YOUR SOC. SEC. NO. |
31. PHYSICIAN’S OR SUPPLIER’S NAME, ADDRESS, ZIP CODE & PHONE NO. |
|||||||||
SIGNED |
DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32. YOUR PATIENT’S ACCOUNT NO. |
|
33. |
YOUR EMPLOYER ID NO |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*PLACE OF SERVICE CODES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
5- DAYCARE FACILITY (PSY) |
|||||||||||||
|
6- NIGHT CARE FACILITY (PSY) |
9- AMBULANCE |
B- OTHER MEDICAL/SURGICAL FACILITY |
|||||||||||
*PLEASE USE CURRENT PROCEDURAL TERMINOLOGY CODES FOR SURGERY
| Fact Name | Details |
|---|---|
| Submission Address | The Key Benefit Request form is submitted to Key Benefit Administrators, Inc., located at P.O. Box 2050, Fort Mill, SC 27916-2050. |
| Patient Information | The form requires comprehensive patient information, including the patient’s name, date of birth, and relationship to the insured. |
| Authorized Signature | Both the patient and authorized person must sign the form to authorize payment and release medical information necessary for processing the request. |
| Diagnoses and Procedures | Healthcare providers completing the form must detail diagnoses and procedures, referencing specific codes that relate to the treatment provided. |
| Disability Dates | The form requires dates of total and partial disability, providing clarity on the duration of the patient's inability to work. |
| Insurance Coverage | The form inquires about other health insurance coverage, which may influence the processing of the claim. |
| State-Specific Governing Laws | For certain states, the submission of this form adheres to local laws governing healthcare claims, ensuring compliance with insurance regulations. |
Once the Key Benefit Request form is fully completed, it should be submitted to Key Benefit Administrators, Inc. for processing. Ensure that all sections are filled accurately to avoid any delays in the approval of your request.
The Key Benefit Request form serves as a means for employees to request medical benefits for services rendered. By submitting this form, patients can document essential information about their medical condition, the care received, and their relationship to the insured. It helps ensure that all necessary details are collected to facilitate the processing of claims effectively.
This form is primarily completed by the employee or authorized individual associated with the patient. Essential patient information, such as the patient's name, date of birth, and relationship to the employee, must be provided. Additionally, the physician needs to complete specific sections related to the medical services rendered to ensure that the claim can be accurately processed.
The form requires a variety of information, including:
Completing each section accurately ensures prompt review and processing of the benefits request.
After filling out the form, it needs to be submitted to Key Benefit Administrators, Inc. This can be done by mailing it to their address: P.O. Box 2050, Fort Mill, SC 27916-2050. Ensure that all sections are filled out correctly to avoid delays in processing. Double-checking the submission for completeness is always a good practice.
Once Key Benefit Administrators, Inc. receives the request form, they will review the information provided. The review process will involve verifying the details with the submitted medical documentation. If additional information is needed, they will contact the employee or the medical provider. Upon completion of the evaluation, a determination will be made regarding the benefits coverage, and a notification will be sent to the employee regarding the outcome.
Filling out the Key Benefit Request form requires attention to detail. One common mistake involves incomplete patient information. Each section must be filled out fully, including the patient’s name, date of birth, and address. Omitting even one piece of information can lead to delays in processing the request. It is crucial to ensure that every box that applies is clearly filled in.
Another mistake frequently made is failing to provide proper authorization. When the employee or authorized person signs the form, it should be clear that they authorize the release of medical information necessary to process the request. Without this authorization, the request may be insufficient and result in denial or further delays. Always double-check that the signature and date sections are complete.
People often overlook the importance of accurately reporting the relationship of the patient to the insured party. This section is critical in determining who is eligible for benefits. If this information is unclear or incorrect, it may cause complications in the approval process. Take particular care to select the appropriate option, whether it be “self,” “spouse,” “child,” or another designation.
Lastly, failing to document all health insurance coverage can lead to significant issues. It is essential to note any other health insurance plans that may cover the patient. If this information is not included, it may affect the total benefits that can be claimed. Be thorough when listing existing coverage, as it impacts the calculation of benefits owed.
The Key Benefit Request form is essential for initiating requests for medical benefits. However, several other forms and documents may accompany it to ensure a smooth and complete submission. These documents add clarity to the request and help facilitate a timely review by the administrators. Below are a few important documents frequently utilized alongside the Key Benefit Request form.
In summary, supplementing the Key Benefit Request form with these additional documents enhances the clarity and completeness of the submission. Each of these forms plays a vital role in ensuring that patients receive the medical benefits they are entitled to in an efficient manner. Proper preparation and attention to detail can significantly improve the experience for all parties involved.
The Key Benefit Request form is used to gather essential information regarding a request for benefits related to medical services. Its structure and purpose are similar to several other documents commonly used in healthcare and benefit claims. Here are nine documents that have similarities to the Key Benefit Request form:
When filling out the Key Benefit Request form, it is important to approach the task systematically. Below are eight essential do's and don'ts to ensure a smooth submission process.
Many people hold misconceptions about the Key Benefit Request form. Understanding these can simplify the process and enhance your experience. Here’s a list to clarify.
Clarifying these misconceptions helps in ensuring a smoother filing process. Always refer to updated guidance if you have questions.
Filling out the Key Benefit Request form requires attention to detail. Here are some key takeaways to ensure the process is smooth and effective:
By following these guidelines, you can help ensure that your Key Benefit Request form is completed correctly and submitted efficiently.