The Lilly Cares Cymbalta Refill form is an essential tool for patients seeking assistance in obtaining their prescribed Cymbalta medication at no cost. This nonprofit program, provided by the Lilly Cares Foundation, aims to support eligible individuals who may struggle with the financial burden of their medications. The application process is straightforward, allowing patients to apply online or via a printable form that can be submitted by fax or mail. To qualify, applicants must meet specific criteria, including being a legal resident of the U.S. and having a household income below certain thresholds. The form requires personal information, such as income details and insurance status, and must be completed in conjunction with a healthcare provider’s certification. Once submitted, Lilly Cares reviews the application and notifies the patient and their provider of the outcome. If approved, patients will receive their medication either at home or at their healthcare provider’s office, ensuring that they continue their treatment without interruption. Additionally, the program includes features like automatic prescription refills and the option for text notifications, making it easier for patients to manage their medications. Overall, the Lilly Cares Cymbalta Refill form plays a vital role in enhancing access to necessary medications for those in need.
LILLY CARES® FOUNDATION Patient Assistance Program Application
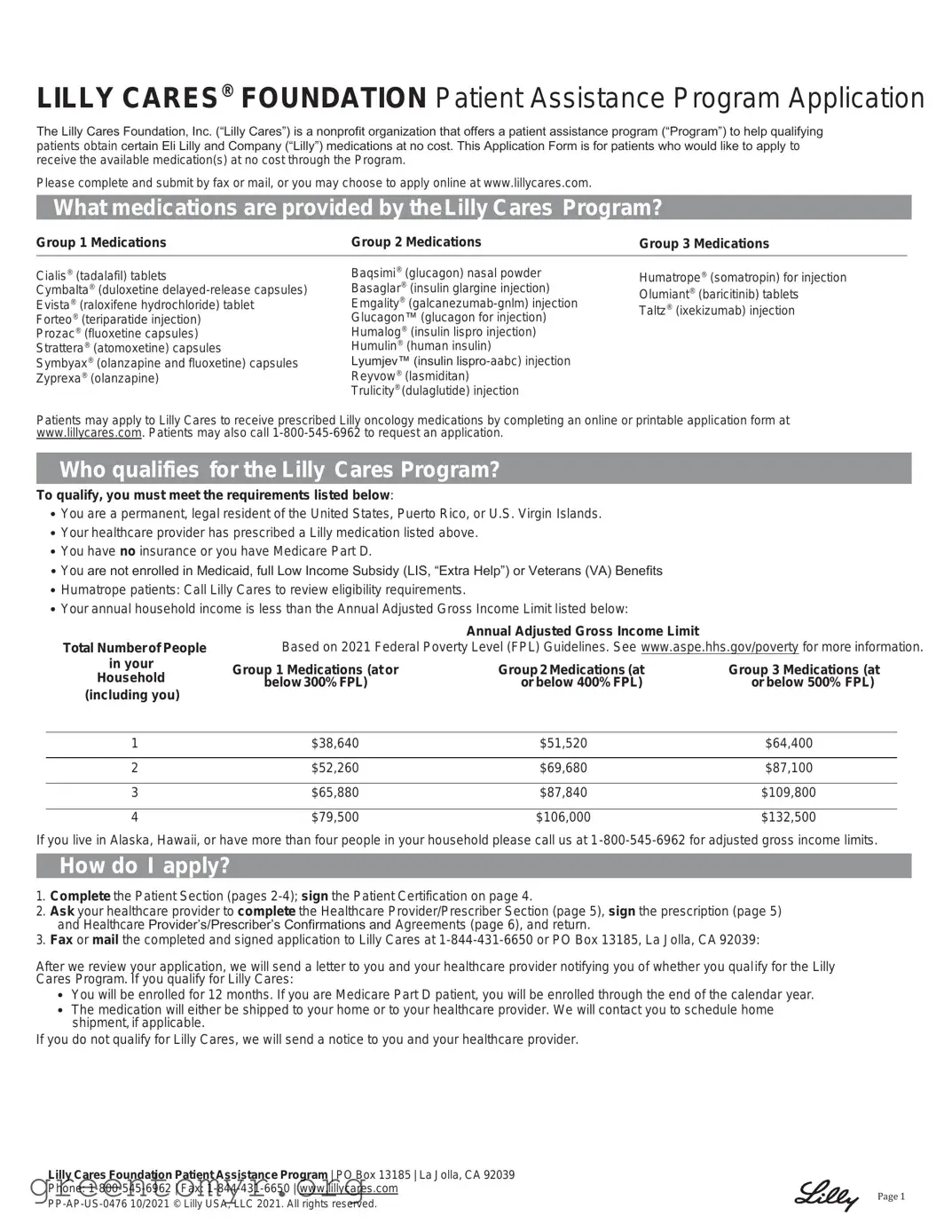
The Lilly Cares Foundation, Inc. (“Lilly Cares”) is a nonprofit organization that offers a patient assistance program (“Program”) to help qualifying patients obtain certain Eli Lilly and Company (“Lilly”) medications at no cost. This Application Form is for patients who would like to apply to receive the available medication(s) at no cost through the Program.
Please complete and submit by fax or mail, or you may choose to apply online at www.lillycares.com.
What medications are provided by the Lilly Cares Program?
Group 1 Medications |
Group 2 Medications |
Group 3 Medications |
|
|
|
Cialis® (tadalafil) tablets
Cymbalta® (duloxetine
Prozac® (fluoxetine capsules) Strattera® (atomoxetine) capsules Symbyax® (olanzapine and fluoxetine) capsules Zyprexa® (olanzapine)
Baqsimi® (glucagon) nasal powder Basaglar® (insulin glargine injection) Emgality®
Lyumjev™ (insulin
Trulicity® (dulaglutide) injection
Humatrope® (somatropin) for injection Olumiant® (baricitinib) tablets Taltz® (ixekizumab) injection
Patients may apply to Lilly Cares to receive prescribed Lilly oncology medications by completing an online or printable application form at www.lillycares.com. Patients may also call
Who qualifies for the Lilly Cares Program?
To qualify, you must meet the requirements listed below:
•You are a permanent, legal resident of the United States, Puerto Rico, or U.S. Virgin Islands.
•Your healthcare provider has prescribed a Lilly medication listed above.
•You have no insurance or you have Medicare Part D.
•You are not enrolled in Medicaid, full Low Income Subsidy (LIS, “Extra Help”) or Veterans (VA) Benefits
•Humatrope patients: Call Lilly Cares to review eligibility requirements.
•Your annual household income is less than the Annual Adjusted Gross Income Limit listed below:
Total Number of People
in your
Household (including you)
Annual Adjusted Gross Income Limit
Based on 2021 Federal Poverty Level (FPL) Guidelines. See www.aspe.hhs.gov/poverty for more information.
Group 1 Medications (at or |
Group 2 Medications (at |
Group 3 Medications (at |
below 300% FPL) |
or below 400% FPL) |
or below 500% FPL) |
1 |
$38,640 |
$51,520 |
$64,400 |
|
|
|
|
2 |
$52,260 |
$69,680 |
$87,100 |
|
|
|
|
3 |
$65,880 |
$87,840 |
$109,800 |
|
|
|
|
4 |
$79,500 |
$106,000 |
$132,500 |
If you live in Alaska, Hawaii, or have more than four people in your household please call us at
How do I apply?
1.Complete the Patient Section (pages
2.Ask your healthcare provider to complete the Healthcare Provider/Prescriber Section (page 5), sign the prescription (page 5) and Healthcare Provider’s/Prescriber’s Confirmations and Agreements (page 6), and return.
3.Fax or mail the completed and signed application to Lilly Cares at
After we review your application, we will send a letter to you and your healthcare provider notifying you of whether you qualify for the Lilly Cares Program. If you qualify for Lilly Cares:
•You will be enrolled for 12 months. If you are Medicare Part D patient, you will be enrolled through the end of the calendar year.
•The medication will either be shipped to your home or to your healthcare provider. We will contact you to schedule home shipment, if applicable.
If you do not qualify for Lilly Cares, we will send a notice to you and your healthcare provider.
Lilly Cares Foundation Patient Assistance Program | PO Box 13185 | La Jolla, CA 92039
Phone:
Page 1
PATIENT SECTION
All fields are required. Please print clearly.
Patient Name: (Last) |
|
|
|
(First) |
|
|
|
|
|
|
|
(MI) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of Birth: |
|
|
|
Preferred |
|
|
|
|
|
|
|
|
|
|
(Month/Day/Year) |
|
|
|
Phone: |
( |
|
|
) |
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
City: |
|
|
|
State: |
|
Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Where would you like your medication delivered? * |
To my home |
To my healthcare provider’s office |
|
|
|
|
||||||||
*Consult with your healthcare provider to confirm delivery location.
Patient Income Information
Number of persons living in your household (including you and all family members):
Annual household income before taxes (include wages, Social Security payments, disability and/or unemployment benefits, pensions, and any other income of yourself and those in your household) *:
*When processing your application, Lilly Cares may contact you and require that you provide documentation showing your income.
Insurance Information
Do you have insurance? (check all that apply)
None |
Medicare Part D |
Medicaid |
|
VA or Military |
Private Insurance (excluding Medicare Part D) |
Other |
|
Authorization to Receive Text Message Notification [Optional]
If your application is approved, we can send you text messages about the Program throughout your enrollment period. These text messages are optional. You can participate in Lilly Cares without signing up for text messages.
When you sign up for the text messages (by providing your cell phone number below), you must agree to the following conditions:
•Lilly Cares will send an autodialed,
•You can opt out at any time by calling
•Lilly Cares is not responsible if a communication is not delivered due to technical difficulties like server issues, phone carrier outages, or discontinued service.
•Be aware that anyone who can open or have access to your phone might see your text messages.
•If your mobile operator is not participating in this service you will not receive messages.
•These text messages are NOT reminders to take your medication. You are responsible to take your medication as prescribed.
•Do NOT report product complaints or adverse events (like side effects) by text message. To report these, please call The Lilly Answers Center at
To receive text messages, you must provide your cell phone number:
Authorization for Automatic Prescription Refills
Our
Yes, automatically fill my medication when I am due for a refill.
No, do not automatically refill my medication. I will call Lilly Cares when I am due for a refill.
Authorization to Speak with Authorized Representative [Optional]
You may provide the names of one or more people with whom you authorize Lilly Cares to speak with on your behalf about this application or your participation in the Lilly Cares Program.
These people can provide or receive your personal information as necessary until you terminate their authority. Their authority will not automatically terminate once we process your application. Their authority will terminate at the end of your enrollment period.
By providing the name(s) below, you certify that individuals are aware and agree that you will provide their name to Lilly Cares for the purpose of serving as your authorized representative.
1. Print Name of Authorized Representative |
|
2. Print Name of Authorized Representative |
You can remove Authorized Representative(s) at any time by calling Lilly Cares at
Lilly Cares Foundation Patient Assistance Program | PO Box 13185 | La Jolla, CA 92039
Phone:
Page 2

Privacy Notice:
We may use and save your personal information to meet legal or regulatory obligations that are in the legitimate interest of Lilly Cares, to fulfill legitimate and lawful business purposes in accordance with Lilly Cares’ record retention policies and applicable laws and regulations, and to respond to lawful requests by public authorities, including to comply with national security or law enforcement requests.
We may transmit personal information about you to Lilly and its affiliates worldwide (who may be assisting with the administration of Lilly
Cares). These affiliates may in turn transmit personal information about you to other Lilly affiliates. Some of Lilly’s affiliates may be located in countries that do not ensure the same level of data protection. Nevertheless, all of Lilly’s affiliates are required to treat personal information in
a manner consistent with this notice. To obtain additional information about privacy practices, including the basis for transfers and safeguards in place for
We provide reasonable physical, electronic and procedural safeguards to protect information we work with and maintain. We limit access to your information to authorized employees, agents, contractors, vendors, subsidiaries, and business partners, or others who need such access
to information to carry out their assigned roles and responsibilities on behalf of Lilly Cares. Please be aware, although we try to protect the information we work with and maintain, no security system can prevent all potential security breaches. We do not sell personal information.
Upon verification, you have the right to request information from us regarding how your personal information is being used and with whom that information is being shared. You also have the right to request to see and get a copy of the personal information that we have about you, request its correction or request its erasure/deletion.
There may be exceptions that apply to your request.
In limited circumstances, you may have the right to have your information transmitted to another entity or person in a
To exercise your rights, you or your authorized representative may submit a request by contacting us using one of the methods listed below.
You may make any of the above requests by contacting us at:
Lilly Cares Foundation Patient Assistance Program
PO Box 13185
La Jolla, CA 92039
Phone:
If you wish to raise a complaint on how we have handled your personal information, you can contact the Global Privacy Office and Data Protection Officer at [email protected] who will investigate the matter for Lilly Cares.
If you are not satisfied with our response or have any concerns about how your data is being processed you can register a complaint with a relevant regulatory authority (e.g., a Data Protection Authority (DPA) or Attorney General).
Lilly Cares Foundation Patient Assistance Program | PO Box 13185 | La Jolla, CA 92039
Phone:
Page 3
PATIENT CERTIFICATION (AGREEMENT)
I understand that:
•Lilly Cares will decide if I qualify for the Program. I understand that my application might not be approved.
•Lilly Cares may change or end the Program, or terminate my enrollment in the Program, at any time.
•Lilly Cares does not charge a fee to apply for participation in the Program. I am not required to use a third party who charges a fee to help with my enrollment, and if I use a third party who charges a fee to help with my enrollment or refills of my medication, this money is not paid to Lilly Cares.
•If approved, my enrollment in the Program will expire at the end of the calendar year (if I am a Medicare Part D patient) or after 12 months. After my enrollment expires, I will need to reapply to the Program.
I certify (agree) that:
•I am a permanent, legal resident of the United States, Puerto Rico, or U.S. Virgin Islands.
•My application is complete and accurate. I have been truthful about my insurance coverage and income.
•I will promptly provide documentation supporting the information I have provided in this application (e.g., income verification documents) if such documentation is requested by Lilly Cares. (Failure to promptly provide complete and accurate documentation when requested may result in immediate termination of application review or removal from the Program if application has already been approved).
•I authorize the Lilly Cares Program Representatives to obtain a consumer report about me in conjunction with my application. Lilly Cares may use my name, date of birth, and address to obtain my consumer report including, but not limited to, information regarding my household size and income. My consumer report will be used to estimate my household income as part of the process to decide if I am eligible for the Program. This inquiry will not impact my credit score. Upon request, Lilly Cares will provide me the name and address of the consumer reporting agency that provides the credit information. I may call Lilly Cares at
•If my application is approved:
o I will notify Lilly Cares of changes to my income or insurance status.
o I will not submit any claim for reimbursement to any third party or government insurer for any product provided to me through the Lilly Cares Program.
o If I have Medicare Part D coverage, I will not seek to have the cost/value associated with the medication I receive through the Program counted as
o If I have Medicare Part D coverage, I will inform my Part D Plan about my enrollment in Lilly Cares. o I will not sell, trade, or transfer any medication I receive through the Program.
I consent to the sharing, use, and receipt of information about me, as described:
To run Lilly Cares, Lilly Cares needs some information about you. When you sign below, you are authorizing any pharmacy, healthcare provider, and or others who are in possession of your personal information, including health information, to share information about you with Lilly Cares, Lilly, and their affiliates, employees, agents, vendors, and business partners who may be assisting with the administration of Lilly Cares (“Receiving Entities”), including health information; in addition, you understand and are authorizing the Receiving Entities to share, use, and disclose your information for the purposes of operating the program.
The Receiving Entities may receive, share, and use the following information:
•Information in this application.
•Information about your medical conditions, treatment, current and future medications, and insurance information.
•Other information the Receiving Entities may obtain to operate Lilly Cares.
•The Receiving Entities may share your information with your healthcare providers and pharmacists.
•Your healthcare providers and pharmacists may share your information with the Receiving Entities.
The Receiving Entities may share your information for the following purposes:
•To review your application to determine your eligibility and to contact you or your healthcare provider, if necessary, for that review.
•To help operate Lilly Cares and for the Receiving Entities’ internal purposes involving other patient assistance and charitable programs.
•To your pharmacies and healthcare providers relating to your participation in Lilly Cares, including personal information and information about your prescription medications.
•Track use of medication.
•To measure program performance and make program improvements.
•We only ask for and share the PHI that we need to operate the program. We do not ask for any PHI that we don’t need, but we may receive some in health records sent to us.
•You don’t have to give permission to share your PHI with Lilly Cares, but we may not be able to assist you without it.
By my signature below, I also agree to the following:
•This authorization allows those who rely on it to release my Protected Health Information for 1 year from the date I have signed it.
•After your PHI has been shared, it may no longer be covered by federal and state privacy laws (such as HIPAA), and it may be shared again.
•I understand that I can cancel my consent at any time by sending a written notice to Lilly Cares at the address on this application. If I cancel my consent, I will no longer qualify for Lilly Cares. My healthcare providers will no longer share my PHI with the Receiving Entities after the date that the Receiving Entities receive and process my cancellation letter, but this will not affect information or disclosures shared before that time. Additionally, once my cancellation is received and processed by the Receiving Entities, my participation in Lilly Cares will be terminated, and after my participation
is terminated, the Receiving Entities will only maintain and use my information for legal and regulatory purposes.
•I have been provided a copy of this authorization.
Patient or Legal Guardian Signature: |
|
Date: |
|||
|
|
|
(SIGNATURE REQUIRED) |
|
|
Patient Printed Name: |
|
|
|
|
|
Lilly Cares Foundation Patient Assistance Program | PO Box 13185 | La Jolla, CA 92039
Phone:
Page 4
HEALTHCARE PROVIDER/PRESCRIBER SECTION
Patient Information (all fields are required):
Note: If the patient’s application is approved, medication will be delivered to the location selected by the patient in the p atient section of this application (page 2). Please coordinate with your patient to ensure appropriate delivery location.
Patient Name: |
|
|
|
|
Date of Birth: |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
Phone: |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
City: |
|
|
|
|
State: |
|
Zip Code: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Drug Allergies: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other Medications: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Rx: I authorize Lilly Cares to act on my behalf for the purpose of transmitting this prescription to the appropriate pharmacy. |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Medication: |
|
|
|
Strength: |
|
|
|
|
Today’s date: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Directions (Please Print): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Quantity to be |
4 months (max) |
|
3 months |
2 months |
|
|
1 month |
||||
Dispensed: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Refills #: |
|
(up to one year of treatment) |
Maximum dose per day: |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
If prescribing insulin, confirm formulation (required): |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|||||
Vial (not available for Basaglar®, Humalog® |
|
|
|
|
|
|
|||||
KwikPen® (not available for Humulin® R 100 units/mL) |
|
|
|
|
|
|
|
|
|||
Cartridge (only available for Humalog® 100 units/mL) |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
Your state may require that prescriptions follow certain content requirements or use a particular form. By signing below, you certify that you are abiding by laws applicable to prescriptions and authorized prescribers in the states in which you are prescribing. I authorize Lilly Cares to act on my behalf for the limited purposes of transmitting this order for prescription medication.
Prescriber Signature:
Dispense as written |
Substitution/brand exchange permitted |
Rubber stamps, signature by other office personnel for the prescriber, and
Healthcare Provider Information (all fields are required):
Printed Prescriber Name and Title: |
|
DEA # (as required): |
|
|
||
|
|
|
|
|
|
|
State License # and State: |
|
NPI #: |
|
|
||
|
|
|
|
|
|
|
Phone: |
|
|
Fax: |
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
City: |
|
|
State: |
|
Zip Code: |
|
|
|
|
|
|
|
|
Office Contact Name: |
|
|
Office Contact Phone: |
|
|
|
|
|
|
|
|
|
|
Lilly Cares Foundation Patient Assistance Program | PO Box 13185 | La Jolla, CA 92039
Phone:
Page 5
Healthcare Provider’s/Prescriber’s Confirmations and Agreements:
By signing below, I (the “Prescriber”) certify to the following statements:
•I prescribed the
•When requested by or required for my Patient and in accordance with his/her needs, Lilly Cares agrees, to the extent consistent with its tax exempt purposes, qualified under Section 170(e)(3) of the Internal Revenue Code, and authorized by Lilly Cares policies, to provide medications to Prescriber for the sole purpose of caring for the ill, needy, indigent, and/or infants in the United States (including Puerto Rico and U.S. Virgin Islands). If Medication is shipped to my office, I will accept the Medication from Lilly Cares and deliver the Medication only to the Patient named on this form. I will provide this Medication at no charge of any kind. I will not use any of the Medication for any other purpose. This Medication will not be offered for sale, trade, or barter; returned for credit; nor will reimbursement be sought or claims be made for the Medication to any third party, including, but not limited to Medicare, Medicaid, or any benefit provider.
•I understand that fax communications sent to a single number may split to multiple Receiving Entities for the purpose of operating the Program.
•Prior to signing this form, I have ensured the Patient is aware of, has consented to, and has directed my disclosure of their information to Lilly Cares so that Lilly Cares may contact the patient to further enable services for those purposes and that such consent and direction applies to disclosures made through the duration of the patient therapy.
•I will give Lilly Cares 90 days advance notice if I need to assign this agreement, in full or in part, to another Prescriber.
•I am a licensed prescriber, and I will comply with and abide by the dispensing laws applicable to the state in which I am prescribing, receiving, storing, and dispensing the Medication. I also will comply with applicable laws related to disposal of, and will properly dispose, unused Medication.
•I understand that Lilly Cares has the right to revise or terminate the Program at any time.
•The information I provided is accurate to the best of my knowledge.
My signature below attests to my understanding and agreement to the above program requirements.
Prescriber Signature: |
|
Date: |
Name of prescriber:
Please print name
Name of Lilly Cares applicant: |
|
DOB: |
Please print name
Lilly Cares Foundation Patient Assistance Program | PO Box 13185 | La Jolla, CA 92039
Phone:
Page 6
| Fact Name | Fact Details |
|---|---|
| Program Purpose | The Lilly Cares Foundation offers a patient assistance program to help eligible patients obtain certain Eli Lilly medications at no cost. |
| Eligibility Criteria | Applicants must be permanent residents of the U.S., Puerto Rico, or U.S. Virgin Islands, have a prescribed Lilly medication, and meet specific income limits. |
| Application Process | Patients can apply online or submit a printed application by fax or mail. The application must be completed by both the patient and their healthcare provider. |
| Annual Income Limits | Income limits vary by household size and medication group, with specific thresholds based on the 2021 Federal Poverty Level. |
| State-Specific Requirements | Some states may have additional laws governing prescription requirements. Providers must comply with local regulations when submitting prescriptions. |
Filling out the Lilly Cares Cymbalta Refill form is a straightforward process. Follow the steps carefully to ensure your application is complete. Once submitted, Lilly Cares will review your application and notify you of your eligibility for the program.
The Lilly Cares Cymbalta Refill form is part of the Lilly Cares Foundation’s Patient Assistance Program. This program aims to help eligible patients obtain Cymbalta (duloxetine) at no cost. To participate, patients need to complete the application form, which can be submitted online, via fax, or by mail. Once submitted, Lilly Cares will review the application and notify the patient and their healthcare provider about their eligibility. If approved, the medication will be shipped to the patient’s home or healthcare provider's office.
Eligibility for the Lilly Cares Program is based on several criteria. Applicants must be permanent, legal residents of the United States, Puerto Rico, or the U.S. Virgin Islands. A healthcare provider must prescribe Cymbalta, and applicants should have no insurance or only Medicare Part D. Additionally, individuals enrolled in Medicaid, full Low Income Subsidy (LIS), or Veterans (VA) Benefits are not eligible. Income limits apply based on household size, and applicants must provide documentation if requested.
Applying for the Lilly Cares Program involves a few straightforward steps:
After submission, Lilly Cares will review the application and inform you and your healthcare provider about your eligibility status.
If your application is approved, you will be enrolled in the program for 12 months. For patients with Medicare Part D, enrollment lasts until the end of the calendar year. The prescribed medication will be shipped either to your home or to your healthcare provider, based on your preference indicated in the application. If you do not qualify, you will receive a notification explaining the decision.
Completing the Lilly Cares Cymbalta Refill form can be a straightforward process, but there are common mistakes that applicants often make. Awareness of these errors can significantly enhance the chances of a successful application. One frequent mistake is failing to provide complete personal information. All fields in the Patient Section are mandatory. Omitting details such as the patient's full name, date of birth, or contact information can lead to delays or outright rejection of the application.
Another common error involves inaccuracies in income reporting. Applicants must provide their annual household income, which should include all sources of income, such as wages, Social Security payments, and disability benefits. Misrepresenting income, even unintentionally, can disqualify an applicant from the program. It is essential to ensure that the information matches any documentation that may be requested later.
Many applicants also overlook the requirement for their healthcare provider to complete and sign specific sections of the form. The Healthcare Provider/Prescriber Section is crucial for verifying the prescription and confirming eligibility. Without a proper signature from the healthcare provider, the application cannot proceed. Thus, it is advisable to communicate with the provider beforehand to ensure all necessary steps are completed.
Furthermore, applicants sometimes misunderstand the delivery options for their medication. The form asks whether the medication should be sent to the patient's home or to the healthcare provider's office. Not consulting with the healthcare provider about the preferred delivery location can lead to complications in receiving the medication. It is important to clarify this detail to avoid any interruptions in treatment.
Another mistake occurs when applicants fail to check their insurance status accurately. The form requires applicants to disclose their insurance coverage, including whether they have Medicare Part D, Medicaid, or private insurance. Misreporting this information can lead to disqualification, as the program has specific eligibility criteria regarding insurance coverage.
In addition, some individuals do not take the time to read the authorization sections carefully. There are critical agreements regarding the sharing of personal health information. Failing to understand these sections can lead to issues later on. Applicants should ensure they are comfortable with the terms before signing.
Moreover, it is important to remember that the application must be submitted with all required documentation. Some applicants mistakenly believe they can send the form without additional proof of income or other necessary documents. This oversight can result in a delay or denial of the application, so it is vital to include all requested materials when submitting the form.
Lastly, applicants sometimes neglect to keep a copy of their completed application. This can be problematic if there are follow-up questions or if documentation is requested later. Retaining a copy allows for easy reference and ensures that applicants can respond promptly to any inquiries from Lilly Cares.
By being mindful of these common mistakes, individuals can navigate the Lilly Cares Cymbalta Refill form more effectively, ensuring a smoother application process and a greater likelihood of receiving the necessary medication.
The Lilly Cares Cymbalta Refill form is an essential document for patients seeking assistance with their medication. However, there are several other forms and documents that may accompany this application to ensure a smooth process. Each of these documents plays a vital role in verifying eligibility and facilitating the necessary approvals.
These documents, when used in conjunction with the Lilly Cares Cymbalta Refill form, help streamline the application process. They ensure that patients receive the assistance they need promptly and efficiently, allowing them to focus on their health and well-being.
The Lilly Cares Cymbalta Refill form shares similarities with several other documents that are designed to assist patients in accessing medications and managing their healthcare needs. Below is a list of eight documents that resemble the Lilly Cares form, along with explanations of their similarities:
Each of these documents serves a specific purpose in helping patients navigate their healthcare options, much like the Lilly Cares Cymbalta Refill form aims to do. Understanding these similarities can empower patients to access the resources they need effectively.
When filling out the Lilly Cares Cymbalta Refill form, here are five important dos and don'ts to keep in mind:
Misconceptions about the Lilly Cares Cymbalta Refill Form
This is not entirely accurate. While income limits apply, the program also considers other factors such as insurance status and residency. Patients with varying income levels may still qualify.
This is false. Patients can complete the application online, by fax, or by mail. Convenience is a priority, and multiple submission methods are available.
This is incorrect. Each application undergoes a review process. Approval depends on meeting specific eligibility criteria set by the Lilly Cares Program.
This is misleading. Enrollment lasts for a fixed period, typically 12 months. Patients must reapply after this period to continue receiving assistance.
Here are some important points to remember when filling out and using the Lilly Cares Cymbalta Refill form: