The Loyal American Claim form is a vital document designed to facilitate the claims process for policyholders seeking benefits from Loyal American Life Insurance Company. This form specifically addresses claims related to early detection benefits for cancer screening tests, ensuring that patients receive the support they need during critical times. Key components of the form include essential information such as the policy number, patient details, and the relationship of the patient to the primary insured. Additionally, it requires the submission of a doctor’s bill that outlines the services performed, the date of service, and the charges incurred. To safeguard the confidentiality of sensitive health information, the form includes an authorization section, allowing healthcare providers to share necessary details with the insurance company for claim processing. Clear instructions guide users through the completion of the form, emphasizing the importance of accuracy and honesty in the information provided. The form also outlines potential consequences for fraudulent claims, reinforcing the seriousness of the claims process. With a dedicated toll-free number for assistance, the Loyal American Claim form aims to streamline the submission process while ensuring that policyholders can access their entitled benefits efficiently.
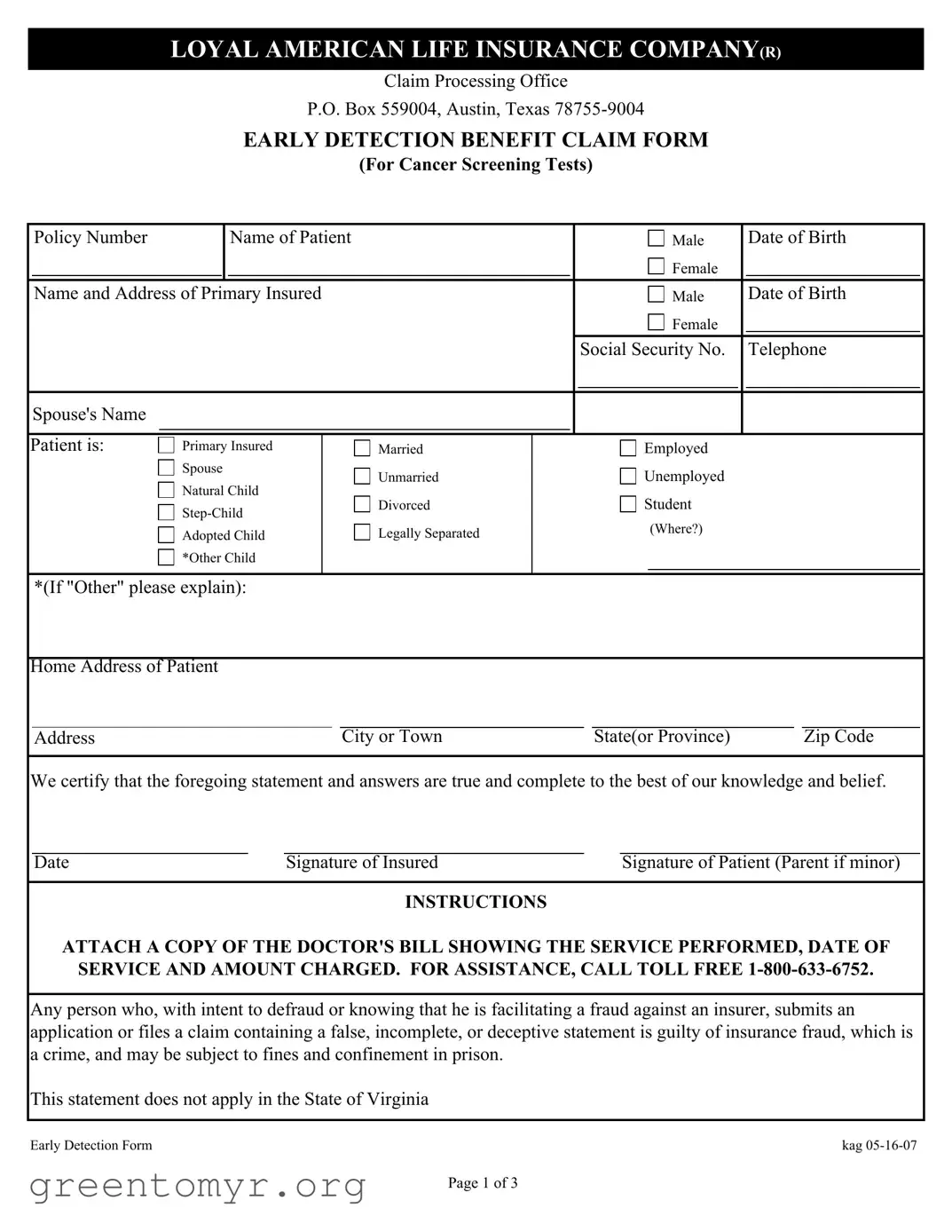
LOYAL AMERICAN LIFE INSURANCE COMPANY(R)
Claim Processing Office
P.O. Box 559004, Austin, Texas
EARLY DETECTION BENEFIT CLAIM FORM
(For Cancer Screening Tests)
|
Policy Number |
|
|
Name of Patient |
|
|
|
Male |
|
Date of Birth |
|
|
|
|
|
|
|
|
|
|
Female |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name and Address of Primary Insured |
|
|
|
Male |
|
Date of Birth |
|
||||
|
|
|
|
|
|
|
|
Female |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Social Security No. |
|
Telephone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Spouse's Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
||||
Patient is: |
Primary Insured |
Married |
|
|
Employed |
|
|
|||||
|
|
Spouse |
Unmarried |
|
|
Unemployed |
|
|
||||
|
|
Natural Child |
|
|
|
|
||||||
|
|
Divorced |
|
|
Student |
|
|
|||||
|
|
|
|
|
|
|||||||
|
|
|
|
|
(Where?) |
|
|
|||||
|
|
Adopted Child |
Legally Separated |
|
|
|
|
|||||
|
|
*Other Child |
|
|
|
|
|
|
|
|
||
*(If "Other" please explain):
Home Address of Patient |
|
|
|
Address |
City or Town |
State(or Province) |
Zip Code |
We certify that the foregoing statement and answers are true and complete to the best of our knowledge and belief.
Date |
Signature of Insured |
Signature of Patient (Parent if minor) |
INSTRUCTIONS
ATTACH A COPY OF THE DOCTOR'S BILL SHOWING THE SERVICE PERFORMED, DATE OF SERVICE AND AMOUNT CHARGED. FOR ASSISTANCE, CALL TOLL FREE
Any person who, with intent to defraud or knowing that he is facilitating a fraud against an insurer, submits an application or files a claim containing a false, incomplete, or deceptive statement is guilty of insurance fraud, which is a crime, and may be subject to fines and confinement in prison.
This statement does not apply in the State of Virginia
Early Detection Form |
kag |
Page 1 of 3
AUTOHORIZATION FORM FOR DISCLOSURES OF A CLAIMANT'S PROTECTED HEALTH INFORMATION
I hereby authorize the disclosure of protected health information about me as described below.
1. The Company, as used in this authoriztion, shall mean:
Great American Life Insurance Company's (R) Long Term Care Division
Loyal American Life Insurance Company (R) United Teacher Associates Insurance Company
2.I authorize all health care providers who have provided treatment or other health care services to me to disclose all information regarding my treatment to the Company's claims and underwriting representatives by and through the Company's contracted agent, Web ISG.
3.The information which is described above will be disclosed to the Company to determine my entitlement to benefits under my health benefits plan or policy.
4.I understand that I may revoke this authorization in writing at any time, except to the extent that action has been taken by the Company in reliance on this authorization, by sending a written revocation to the Company's Claims Department at P.O. Box 26580, Austin, Texas
5.This authorization will expire
6.I understand that the information which will be provided under this authorization is necessary for the Company to evaluate my entitilement to benefits under my health benefits plan or policy and that the Company will condition the provision of payment benefits to me on my providing this authorization, and my claim may be denied if I refuse to provide this authorization.
7.I understand that if the person or entity that receives my protected health information is not a health care provider or health plan covered by the federal privacy regulations, the information may be redisclosed by such person or entity and will likely no longer be protected by the federal privacy regulations. In the case of this authorization, however, the information described above will be received by a health plan which is covered by the federal privacy regulations.
8.I understand that a photocopy, facsimile copy, or electronic copy of this authorization shall be considered as effective and valid as the original.
9.I understand that I or my personal representative am entitled to receive a copy of this authorization upon request.
Page 2 of 3
If you are the representative of the claimant, decribe the scope of your authority to act on the claimant's behalf:
Claimant Name
Name of claimant's personal representative, if applicable
Relationship of personal representative to the claimant
Signature of claimant (or claimant's representative)
Date of claimant's (or claimant's representative) signature
A signed copy of this form will be provided any time upon request.
Page 3 of 3
| Fact Name | Description |
|---|---|
| Company Name | The claim form is for Loyal American Life Insurance Company, which is part of Great American Life Insurance Company's Long Term Care Division. |
| Claim Type | This form is specifically for the Early Detection Benefit Claim related to cancer screening tests. |
| Required Information | Applicants must provide details such as the policy number, patient’s name, date of birth, and social security number. |
| Submission Instructions | To submit a claim, attach a copy of the doctor’s bill showing the service performed, date of service, and amount charged. |
| Governing Law | In Virginia, specific statements regarding insurance fraud do not apply, highlighting state-specific legal considerations. |
After completing the Loyal American Claim form, you will need to submit it along with any required documents to the designated address. This process is essential for ensuring that your claim is processed efficiently and accurately.
The Loyal American Claim Form is primarily used to submit claims for benefits related to cancer screening tests. It allows policyholders to request reimbursement for medical services received, ensuring they can access their benefits when needed.
To fill out the claim form, start by providing your policy number and the patient's details, including their name, date of birth, and relationship to the primary insured. You will also need to include the patient's home address and contact information. Make sure to sign the form to certify that the information provided is true and complete.
When submitting the claim form, you must attach a copy of the doctor's bill. This bill should clearly show the service performed, the date of service, and the amount charged. Without this documentation, your claim may be delayed or denied.
If you require assistance while completing the claim form, you can call the toll-free number at 1-800-633-6752. A representative will be available to help you with any questions or concerns you may have.
Providing false or misleading information on the claim form can lead to serious consequences. It may be considered insurance fraud, which is a crime. If found guilty, you could face fines and even imprisonment. It is crucial to provide accurate and complete information.
The authorization for the disclosure of protected health information is valid for twenty-four (24) months from the date it is signed. After this period, you would need to provide a new authorization if additional information is required.
Yes, you can revoke the authorization in writing at any time. However, if the company has already taken action based on that authorization, your revocation will not affect those actions. To revoke, send a written notice to the Claims Department at the address provided on the form.
If you are acting on behalf of the claimant, you will need to describe the scope of your authority on the claim form. Include your name, relationship to the claimant, and sign the form to confirm your authority to act on their behalf.
Filling out the Loyal American Claim form can be a straightforward process, but many individuals make common mistakes that can delay their claims. One frequent error is failing to provide complete information. Each section of the form requires specific details, such as the policy number and the patient's date of birth. Omitting any of these details can result in the claim being returned for correction, which can prolong the processing time.
Another mistake is not attaching the required documentation. The instructions clearly state that a copy of the doctor's bill is necessary. This bill should show the service performed, the date of service, and the amount charged. Without this essential documentation, the claim may be considered incomplete, leading to further delays in receiving benefits.
People often overlook the importance of signatures. The form requires signatures from both the insured and the patient (or the parent if the patient is a minor). Neglecting to sign the form can render it invalid. It's crucial to double-check that all necessary signatures are included before submitting the claim.
In addition, individuals sometimes misinterpret the authorization section. It’s vital to understand that by signing this section, you are allowing health care providers to share your medical information with the insurance company. Failing to complete this section properly can lead to complications in processing the claim, as the insurance company may need this information to determine eligibility for benefits.
Finally, some people do not keep a copy of the submitted claim form for their records. Having a copy can be invaluable if there are any questions or issues regarding the claim later on. It serves as proof of what was submitted and can help in following up with the insurance company. By avoiding these common mistakes, individuals can help ensure a smoother claims process and receive their benefits in a timely manner.
The process of filing a claim with Loyal American Life Insurance Company can often feel overwhelming. To assist individuals in navigating this journey, several forms and documents are typically required alongside the Loyal American Claim form. Each document serves a specific purpose, ensuring that the claim process is thorough and efficient. Below is a list of these essential forms and documents.
Understanding these documents and their roles can significantly ease the claims process. Each form contributes to a clearer picture of the situation, allowing the insurance company to make informed decisions. By preparing these materials in advance, claimants can help facilitate a smoother experience as they seek the benefits to which they are entitled.
The Loyal American Claim form shares similarities with several other documents related to insurance claims and healthcare authorizations. Below is a list of eight such documents, detailing how they are similar to the Loyal American Claim form:
When filling out the Loyal American Claim form, it's important to follow specific guidelines to ensure your claim is processed smoothly. Here are some things you should and shouldn't do:
Following these guidelines will help ensure that your claim is processed efficiently. If you have questions or need assistance, you can call the toll-free number provided on the form.
Understanding the Loyal American Claim form can be challenging. Here are some common misconceptions:
Clearing up these misconceptions can help ensure a smoother claims process.
When filling out and using the Loyal American Claim form, it is crucial to follow specific guidelines to ensure a smooth claims process. Here are key takeaways to keep in mind:
By adhering to these guidelines, you can help facilitate the processing of your claim and avoid potential pitfalls. Take action promptly to ensure your rights and benefits are protected.