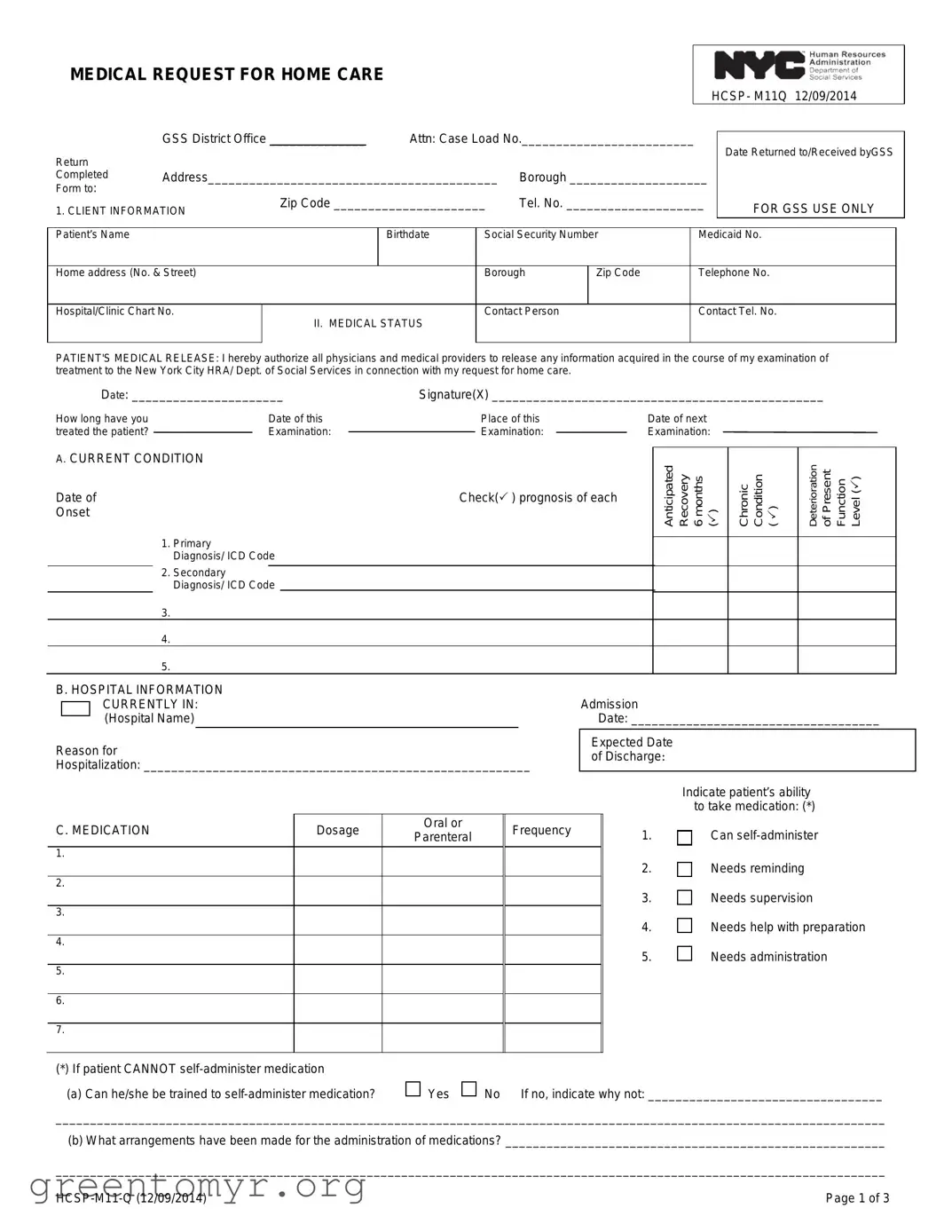
The M11Q form is a crucial document used in the process of requesting home care services for patients in need. This form, officially titled the Medical Request for Home Care, is primarily utilized by healthcare providers to communicate essential medical information about a patient to the appropriate agencies. It captures vital details such as the patient's name, birthdate, and social security number, ensuring that all personal information is accurately documented. The form also requires a thorough medical status report, including primary and secondary diagnoses, prognosis, and medication management. It addresses the patient's current condition, any necessary medical treatments, and the types of assistance they may require at home. Additionally, the M11Q form facilitates communication about equipment needs and referrals to home care agencies. Importantly, it mandates a physician's certification, confirming that the patient can be cared for at home and that their medical needs are clearly outlined. This structured approach not only streamlines the process for obtaining home care but also prioritizes the patient's individual requirements and circumstances.

MEDICAL REQUEST FOR HOME CARE |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
HCSP- M11Q 12/09/2014 |
||
|
GSS District Office ______________ |
Attn: Case Load No._________________________ |
|
|
|
|
||||||
Return |
|
|
Date Returned to/Received byGSS |
|||||||||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
Completed |
Address__________________________________________ |
Borough ____________________ |
|
|
|
|||||||
Form to: |
|
Zip Code ______________________ |
Tel. No. ____________________ |
|
|
|
||||||
1. CLIENT INFORMATION |
|
FOR GSS USE ONLY |
||||||||||
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|||
Patient’s Name |
|
|
|
Birthdate |
Social Security Number |
|
Medicaid No. |
|||||
|
|
|
|
|
|
|
|
|
||||
Home address (No. & Street) |
|
|
|
Borough |
Zip Code |
|
Telephone No. |
|||||
|
|
|
|
|
|
|
|
|
||||
Hospital/Clinic Chart No. |
II. MEDICAL STATUS |
Contact Person |
|
|
Contact Tel. No. |
|
||||||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT'S MEDICAL RELEASE: I hereby authorize all physicians and medical providers to release any information acquired in the course of my examination of treatment to the New York City HRA/ Dept. of Social Services in connection with my request for home care.
Date: ______________________ |
Signature(X) ________________________________________________ |
|||||
How long have you |
|
Date of this |
|
Place of this |
|
Date of next |
treated the patient? |
|
Examination: |
|
Examination: |
|
Examination: |
|
|
|
||||
A. CURRENT CONDITION
Date of
Onset
1. Primary
Diagnosis/ ICD Code
2. Secondary
Diagnosis/ ICD Code
3.
4.
5.
Check( ) prognosis of each
Anticipated Recovery 6 months ()
Chronic Condition ( )
Deterioration of Present Function Level ()
B. HOSPITAL INFORMATION |
|
|
|
|
|
|
|
|||
|
|
CURRENTLY IN: |
|
|
|
|
Admission |
|
||
|
|
|
|
|
|
|
||||
|
|
(Hospital Name) |
|
|
|
|
|
Date: ____________________________________ |
||
|
|
|
|
|
|
|||||
Reason for |
|
|
|
|
Expected Date |
|
||||
|
|
|
|
of Discharge: |
|
|||||
Hospitalization: ________________________________________________________ |
|
|||||||||
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
Indicate patient’s ability |
|
|
|
|
|
|
|
|
|
|
to take medication: (*) |
C. MEDICATION |
Dosage |
Oral or |
Frequency |
|
1. |
Can |
||||
Parenteral |
|
|||||||||
|
|
|
|
|
|
|
|
|||
1. |
|
|
|
|
|
|
|
2. |
Needs reminding |
|
|
|
|
|
|
|
|
|
|
||
2. |
|
|
|
|
|
|
|
3. |
Needs supervision |
|
|
|
|
|
|
|
|
|
|
||
3. |
|
|
|
|
|
|
|
4. |
Needs help with preparation |
|
|
|
|
|
|
|
|
|
|
||
4. |
|
|
|
|
|
|
|
5. |
Needs administration |
|
|
|
|
|
|
|
|
|
|
||
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(*)If patient CANNOT
(a)Can he/she be trained to
Yes
No If no, indicate why not: __________________________________
________________________________________________________________________________________________________________________
(b)What arrangements have been made for the administration of medications? _______________________________________________________
________________________________________________________________________________________________________________________
Page 1 of 3 |
D. MEDICAL TREATMENT |
Does the patient receive any of the following medical treatment? |
Yes |
No |
||||||||
|
|
Indicate medical treatment currently received: ( ) |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
1. |
Decubitus Care |
|
7. Colostomy Care |
|
15. |
Suctioning |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
2. |
Dressings: Sterile |
|
8. |
Ostomy Care |
|
16. |
Speech/Hearing/ Therapy |
|
|||
|
Simple |
|
|
|
|
|
|
|
|
|
|
|
|
9. |
Oxygen Administration |
|
17. |
Occupational Therapy |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
3. |
Bed bound Care (turning, |
|
10. |
Catheter Care |
|
18. |
Rehabilitation Therapy |
|
|||
|
exercising, positioning) |
|
|
|
|
|
|
|
|
|
|
|
11. |
Tube Irrigation |
|
19. |
Indicate any special |
|
|||||
|
|
|
|
|
|
|
|
|
|
dietary needs |
|
4. |
Ambulation Exercise |
|
12. |
Monitor Vital Signs |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
5. |
ROM/Therapeutic Exercise |
|
13. |
Tube Feedings |
|
20. |
Other |
||||
|
|
|
|
|
|
|
|
|
|
|
|
6. |
Enema |
|
|
14. |
Inhalation Therapy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
For each treatment checked, indicate frequency recommended, how the service is currently being provided and what plans have been made to provide the service in the future: (Attach additional documentation as necessary.)
_____________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________
Based on the medical condition, do you recommend the provision of service to assist with personal care and/or light housekeeping tasks?
Yes
No
Please indicate contributing factors (e.g. limited range of motion, muscular motor impairments, etc.) and any other information that may be pertinent to the patient's need for assistance with personal care services tasks.
_________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________
Can patient direct a home care worker?
Yes
No If no, explain below:
____________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________
E. EQUIPMENT/SUPPLIES
Please indicate which equipment/supplies the client has, needs or has been ordered.
Has Needs Ordered
Cane
Crutches
Walker
Wheelchair
Hospital Bed
Side Rails
Has Needs Ordered
Bedpan/Urinal
Commode
Diapers
Hoyer Lift
Dressings
Respiratory Aids
Has Needs Ordered
Bath Bar
Bath Seat
Grab Bar
Shower Handle
Other (Specify)
If any needed equipment was not ordered, what other plans have been made to meet this need?
_________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________
SSN: _________________________________
Page 2 of 3 |
F. REFERRALS
Has a referral been made to any of these agencies: Certified Home Health Agency,
Facility (HRF), a Skilled Nursing Facility (SNF) or the Lombardi Program? |
Yes |
No |
|
|
*IDENTITY AGENCY |
SERVICE |
|
STATUS OF SERVICE |
REFERRAL DATE |
__________________________________ |
__________________________________ |
__________________________________ |
___________________________________ |
|
__________________________________ |
__________________________________ |
__________________________________ |
___________________________________ |
|
G. ADDITIONAL COMMENTS
Describe any other aspects of the patient’s medical, social, family or home situation which affects the patient‘s ability to function, or may affect need for home care. If necessary, please attach an additional sheet(s) explaining the patient’s condition in greater detail.
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
Signature of Person Completing Additional Comments Section
Title Agency
Date
Physician’s Certification
I, the undersigned physician, certify that this patient can be cared for at home, and that I have accurately described his or her medical condition, needs and regimens, including any medication regimens, at the time I examined him or her. I understand that I am not to recommend the number of hours of personal care services this patient may require. I also understand that this physician’s order is subject to the New York State Department of Health regulations at part 515, 516, 517, and 518 of title 18 NYCRR, which permit the department to impose monetary penalties on, or sanction and recover overpayments from, providers or prescribers of medical care, services or supplies when medical care, services or supplies that are unnecessary, improper or exceed the patient’s documented medical condition are provided or ordered.
|
|
|
|
|
|
|
|
|
|
Intern |
|
|
Resident |
||||
*(PRINT) Physician’s Name |
|
|
Specialty |
|
|
*Physician’s Signature |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
*Business Address |
|
|
|
|
|
|
*City |
|
*State |
|
|
*Zip Code |
|||||
Signature date must be within thirty days after medical exam of patient. |
|
|
|
|
|
|
|
|
|||||||||
______________________ |
________________ |
____________________ |
__________________________________ |
_____________________________ |
|
|
|||||||||||
*Date Form Completed |
*Registry Number |
*NPI Number |
|
|
*Physician’s Telephone |
Physician’s |
|||||||||||
Indicate where form was completed: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
___________________________________ |
________________________________________________________ |
__________________________ |
|||||||||||||||
Hospital/Clinic/Institution Name |
|
Address |
Telephone No. / |
||||||||||||||
If Nurse /Social Worker/other person assisted in completing this form:
______________________________ |
_______________________ |
________________________________________________ |
____________________________ |
Name |
Title |
Address |
Telephone No. / |
*Mandatory |
|
|
|
|
|
Page 3 of 3 |
EIGHT HELPFUL HINTS FOR ACCURATE COMPLETION OF THE MEDICAL
REQUEST FOR HOME CARE (M11Q)
* Please provide this sheet to the physician filling out the Medical Request for Home Care
Eight Helpful Hints for Accurate Completion of the
Medical Request for Home Care
1.The client’s name, address and Social Security number must be provided.
2.The medical professional must complete the
3.The medical professional must not recommend or request the number of hours of personal care services.
4.The
5.The date of the examination must be provided.
6.The physician must sign and date the
7.The registry number, NPI (national provider ID), and the complete business address of the physician must be indicated.
8.The completed signed copy of the
| Fact Name | Description |
|---|---|
| Form Purpose | The M11Q form is used to request home care services for patients requiring medical assistance. |
| Governing Law | This form is governed by New York State Department of Health regulations, specifically parts 515, 516, 517, and 518 of title 18 NYCRR. |
| Patient Information | Essential details such as the patient's name, address, and Social Security number must be included on the form. |
| Physician's Role | A licensed physician must complete and sign the M11Q, certifying the patient's need for home care. |
| Submission Timeline | The completed form must be submitted within 30 days after the patient's medical examination. |
| Signature Requirement | The physician's signature is mandatory and must be dated within 30 days of the examination. |
| Additional Documentation | Additional sheets may be attached to provide more details about the patient's condition or care needs. |
Completing the M11Q form is an essential step in the process of requesting home care services. This form collects vital information about the patient's medical condition, treatment needs, and home care requirements. After filling out the form, it should be submitted to the appropriate agency to ensure timely processing.
The M11Q form, also known as the Medical Request for Home Care, is a document used to request home care services for patients. It is essential for healthcare providers to accurately complete this form to ensure that patients receive the appropriate level of care based on their medical needs. The form collects information about the patient’s medical status, current treatments, and any special requirements for home care services.
The M11Q form must be completed by a licensed physician in New York State. This medical professional is responsible for providing detailed information about the patient’s medical condition, treatment needs, and any recommendations for home care services. It is crucial that the physician does not specify the number of hours of personal care services required, as this is outside the scope of the form.
The M11Q form requires a variety of information, including:
Each section must be filled out accurately to ensure the patient's needs are fully understood.
Once completed, the M11Q form should be submitted to the appropriate office, such as the New York City Human Resources Administration (HRA) or the Department of Social Services. It is important that the form is submitted within 30 calendar days after the medical examination to avoid delays in care.
If the M11Q form is incomplete or lacks necessary signatures, it may be rejected or delayed in processing. This can lead to a significant delay in the patient receiving the home care services they need. Therefore, it is essential for the physician and any assisting personnel to ensure that all required fields are filled out accurately before submission.
Yes, there are several guidelines to follow when completing the M11Q form:
Following these guidelines helps to streamline the process and ensures compliance with regulations.
The M11Q form includes a section to determine whether the patient can direct a home care worker. If the patient is unable to do so, it is important to provide an explanation. This information is crucial for planning appropriate care and support for the patient.
If the patient has special dietary needs, this should be clearly indicated on the M11Q form. The medical professional should provide detailed information about these needs to ensure that home care services can accommodate them. This may include specific dietary restrictions or recommendations that are essential for the patient's health.
There is a section on the M11Q form for additional comments. This is where the medical professional can elaborate on any other aspects of the patient's situation that may impact their ability to function or their need for home care. If necessary, attaching additional sheets can provide more comprehensive information.
Filling out the M11Q form can be a straightforward process, but mistakes can lead to delays or denials in home care services. One common error is failing to provide complete client information. The patient's name, address, Social Security number, and Medicaid number are essential. Omitting any of this information can result in processing issues. Ensure all fields are filled out accurately and legibly to avoid complications.
Another frequent mistake occurs when the medical professional inaccurately describes the patient's medical condition. It is crucial that the medical status section is filled out with precise diagnoses and relevant ICD codes. Incomplete or vague descriptions can lead to misunderstandings about the patient's needs. Providing detailed information about the patient's current condition and prognosis is vital for appropriate care decisions.
People often confuse the role of the physician when filling out the M11Q. The medical professional must not request a specific number of hours for personal care services. This request is outside their purview and can lead to rejection of the form. Instead, the physician should focus on detailing the patient's medical needs without suggesting specific care hours.
Additionally, the M11Q must be signed by a licensed physician in New York State. Failing to secure the proper signature can invalidate the form. It is also important that the physician dates the form within 30 days of the examination. Submitting an undated or outdated form can lead to unnecessary delays in processing.
Lastly, neglecting to include the physician's registry number, NPI, and complete business address is a common oversight. These details are mandatory and must be accurately provided to ensure the form is processed correctly. Double-checking this information before submission can help prevent any issues with the home care request.
The M11Q form is a crucial document for requesting home care services. However, several other forms and documents often accompany it to ensure a comprehensive understanding of the patient's needs and circumstances. Below is a list of these additional forms, each serving a specific purpose in the home care process.
Each of these documents plays a vital role in ensuring that home care services are tailored to meet the unique needs of the patient. Properly completing and submitting these forms can significantly enhance the quality of care provided and ensure compliance with healthcare regulations.
The M11Q form, which is used for medical requests for home care, shares similarities with several other documents in terms of purpose and structure. Below is a list of eight documents that are comparable to the M11Q form:
When filling out the M11Q form, keep the following tips in mind:
This form is designed for a range of patients, including those who may need assistance with daily activities due to chronic conditions or temporary illnesses.
While a licensed physician must sign the form, other medical professionals, such as nurse practitioners, can assist in its completion.
Submitting the form does not automatically ensure that home care services will be provided. Approval is subject to review by the appropriate agency.
The form explicitly states that the medical professional should not recommend the number of hours for personal care services.
The completed form must be submitted within 30 calendar days following the patient's examination to remain valid.
This form is applicable to patients of all ages who require home care services, regardless of their age.
Accurate and thorough medical details are crucial for the assessment of the patient's needs and for the approval of services.
While it is often used for Medicaid applications, the M11Q can be relevant for various insurance and assistance programs that cover home care services.
Filling out the M11Q form can seem daunting, but understanding its key components can simplify the process. Here are some important takeaways to keep in mind:
By following these guidelines, you can help ensure that the M11Q form is filled out correctly and efficiently. This will facilitate a smoother process for obtaining home care services for those in need.