The Medicaid Standing Order form, specifically Form 2015-SO, is designed to facilitate transportation requests for individuals who require regular medical appointments. This form is essential for those who need transportation services three or more times a week for a duration of three months or longer. It captures vital information, including the enrollee's name, date of birth, Medicaid number, and preferred appointment days. The form also details the medically necessary mode of transportation, ranging from livery services to various types of ambulances, based on the enrollee's specific needs. Additionally, it requires information about the preferred transportation provider, pick-up and drop-off locations, and any special directions or needs for the patient. A certification statement at the end of the form ensures that the information provided is accurate and that the requester understands the rules and regulations governing Medicaid-funded travel. For any inquiries, the LogistiCare Facility Services Department can be contacted directly, ensuring support is available throughout the process.
Form
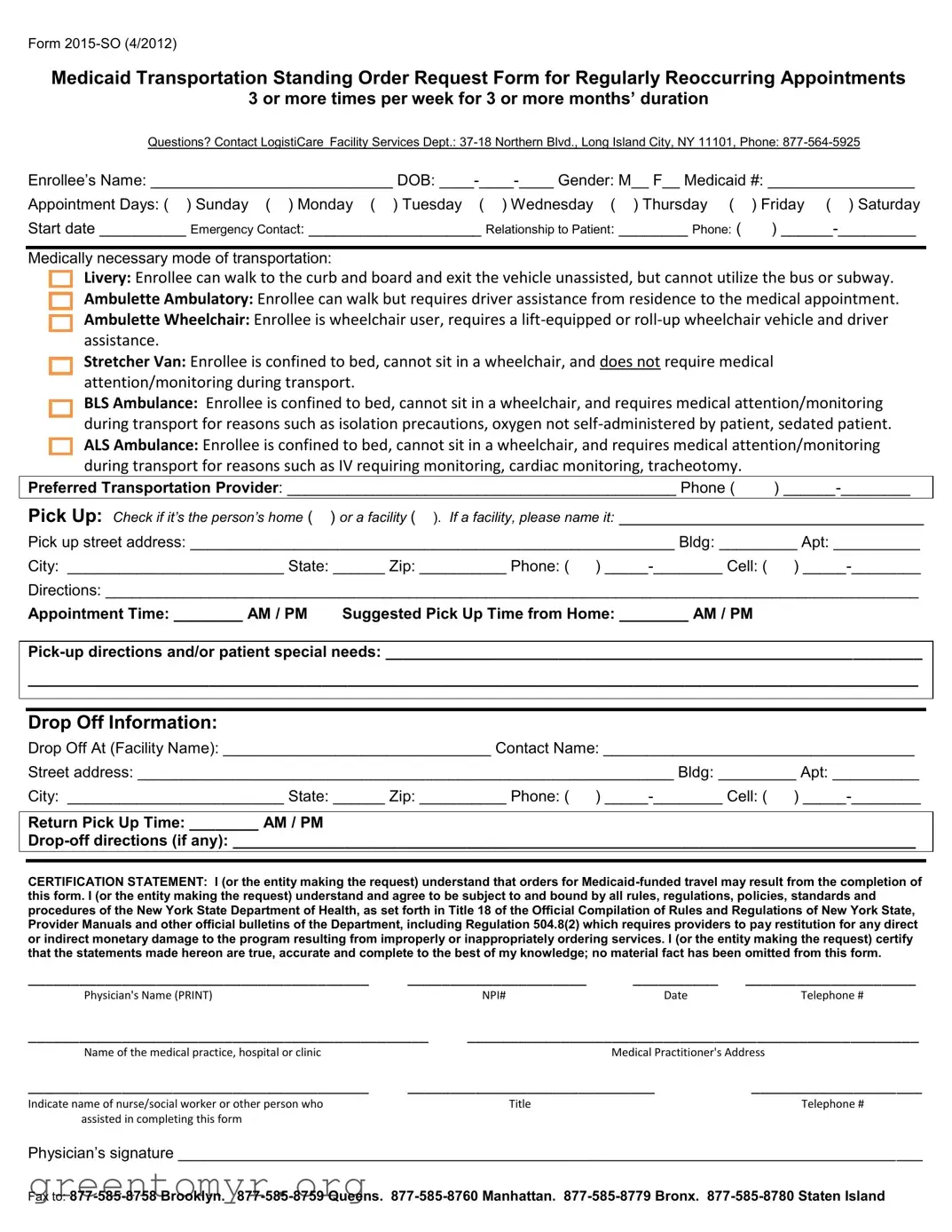
Medicaid Transportation Standing Order Request Form for Regularly Reoccurring Appointments
3 or more times per week for 3 or more months’ duration
Questions? Contact LogistiCare Facility Services Dept.:
Enrollee’s Name: ____________________________ DOB:
Appointment Days: ( ) Sunday ( ) Monday ( ) Tuesday ( ) Wednesday ( |
) Thursday ( |
) Friday ( ) Saturday |
Start date __________ Emergency Contact: ____________________ Relationship to Patient: |
________ Phone: ( |
) |
Medically necessary mode of transportation:
Livery: Enrollee can walk to the curb and board and exit the vehicle unassisted, but cannot utilize the bus or subway.
Ambulette Ambulatory: Enrollee can walk but requires driver assistance from residence to the medical appointment.
Ambulette Wheelchair: Enrollee is wheelchair user, requires a
Stretcher Van: Enrollee is confined to bed, cannot sit in a wheelchair, and does not require medical attention/monitoring during transport.
BLS Ambulance: Enrollee is confined to bed, cannot sit in a wheelchair, and requires medical attention/monitoring during transport for reasons such as isolation precautions, oxygen not
Preferred Transportation Provider: _____________________________________________ Phone ( )
Pick Up: Check if it’s the person’s home ( ) or a facility ( ). If a facility, please name it: ________________________________
Pick up street address: ________________________________________________________ Bldg: _________ Apt: __________
City: _________________________ State: ______ Zip: __________ Phone: ( )
Directions: ______________________________________________________________________________________________
Appointment Time: ________ AM / PM Suggested Pick Up Time from Home: ________ AM / PM
_______________________________________________________________________________________________________
Drop Off Information:
Drop Off At (Facility Name): _______________________________ Contact Name: ____________________________________
Street address: ______________________________________________________________ Bldg: _________ Apt: __________
City: _________________________ State: ______ Zip: __________ Phone: ( )
Return Pick Up Time: ________ AM / PM
CERTIFICATION STATEMENT: I (or the entity making the request) understand that orders for
________________________________________ |
_____________________ |
__________ |
____________________ |
|
Physician's Name (PRINT) |
|
NPI# |
Date |
Telephone # |
_______________________________________________ |
_____________________________________________________ |
|||
Name of the medical practice, hospital or clinic |
|
|
Medical Practitioner's Address |
|
________________________________________ |
_____________________________ |
____________________ |
||
Indicate name of nurse/social worker or other person who |
|
Title |
|
Telephone # |
assisted in completing this form |
|
|
|
|
Physician’s signature ______________________________________________________________________________________
Fax to:
| Fact Name | Description |
|---|---|
| Form Purpose | The Medicaid Transportation Standing Order Request Form is designed for requesting transportation services for enrollees with regularly reoccurring medical appointments, specifically three or more times per week for three or more months. |
| Contact Information | For any inquiries related to the form, individuals can contact LogistiCare Facility Services Department at 877-564-5925 or visit their office located at 37-18 Northern Blvd., Long Island City, NY 11101. |
| Governing Laws | This form is governed by the New York State Department of Health regulations, specifically Title 18 of the Official Compilation of Rules and Regulations of New York State, including Regulation 504.8(2). |
| Certification Statement | The individual completing the form must certify that all information provided is true and complete. They acknowledge understanding of the rules and agree to be bound by the regulations set forth by the New York State Department of Health. |
Once you have the Medicaid Standing Order form in front of you, follow these steps to complete it accurately. Be sure to have all necessary information on hand, including the enrollee's details and appointment specifics.
The Medicaid Standing Order form, specifically Form 2015-SO, is used to request Medicaid transportation for individuals who have regularly recurring medical appointments. This form is particularly relevant for patients who require transportation three or more times a week for a duration of three or more months.
The form should be completed by a physician or a designated medical professional on behalf of the patient. It may also be filled out by a nurse, social worker, or another authorized individual who assists the patient in accessing necessary medical services.
The form allows for various modes of transportation based on the medical needs of the enrollee. Options include:
Each option caters to different levels of assistance required by the patient, from those who can walk unassisted to those who need medical monitoring during transport.
Consider the patient's mobility and medical condition. If the patient can walk but needs assistance, an Ambulette Ambulatory may be suitable. For wheelchair users, an Ambulette Wheelchair is necessary. In cases where the patient is bedridden and requires medical attention, a BLS or ALS Ambulance is appropriate.
The form requires several key pieces of information, including:
Completing all sections accurately is crucial to ensure timely and appropriate transportation services.
Once completed, the form should be faxed to the appropriate number based on the borough. For example, fax numbers vary for Brooklyn, Queens, Manhattan, Bronx, and Staten Island. Make sure to verify the correct fax number before submission to avoid delays.
After submission, the request will be reviewed by the Medicaid transportation provider. If approved, the patient will receive confirmation of their transportation arrangements, including details about pick-up and drop-off times. If there are any issues or additional information needed, the provider will reach out to the contact listed on the form.
Yes, changes can be made if necessary. It is important to contact the transportation provider as soon as possible to update any details such as appointment times or pick-up locations. Prompt communication helps ensure that the patient’s transportation needs are met effectively.
If you have questions or need help completing the form, you can contact the LogistiCare Facility Services Department at 877-564-5925. They can provide guidance and answer any specific questions you may have regarding the Medicaid Standing Order process.
Completing the Medicaid Standing Order form can seem straightforward, but there are several common mistakes that individuals often make. These errors can lead to delays in transportation services or even denial of requests. Understanding these pitfalls can help ensure a smoother process for obtaining necessary medical transportation.
One significant mistake is failing to provide complete information. Each section of the form must be filled out thoroughly. For instance, omitting the enrollee’s Medicaid number or not specifying the appointment days can create confusion. Incomplete forms often result in additional follow-up, which can delay the transportation services needed for medical appointments.
Another frequent error is incorrectly selecting the mode of transportation. It’s crucial to accurately assess the enrollee’s needs. Choosing a mode that does not match the enrollee's condition can lead to inappropriate transportation being arranged. For example, selecting a stretcher van when an ambulette would suffice not only wastes resources but may also cause logistical issues on the day of the appointment.
Additionally, people often overlook the importance of the contact information. Providing accurate contact details for both the enrollee and the drop-off facility is essential. If there are any changes or issues on the day of transport, having the right phone numbers ensures that communication can occur swiftly. Missing or incorrect contact information can lead to missed appointments and frustration for all parties involved.
Finally, individuals sometimes neglect to review the certification statement at the end of the form. This section is crucial, as it confirms that the information provided is accurate and that the requester understands the implications of the request. Failing to sign or date this section can render the entire form invalid, causing further delays in securing transportation services.
The Medicaid Standing Order form is often used in conjunction with several other documents that facilitate the process of obtaining medical transportation and services. Below is a list of forms and documents that are commonly associated with the Medicaid Standing Order form. Each document serves a specific purpose in ensuring that the necessary information is collected and processed efficiently.
These forms and documents work together to create a comprehensive system for managing medical transportation needs under Medicaid. They help ensure that patients receive the appropriate care and support throughout their treatment journey.
The Medicaid Standing Order form shares similarities with several other documents that serve various purposes in healthcare and transportation services. Here’s a list of eight documents that are comparable to the Medicaid Standing Order form:
When filling out the Medicaid Standing Order form, there are important steps to follow. Here’s a list of things you should and shouldn’t do:
This form is designed for regularly occurring appointments, not just emergencies. It facilitates transportation for ongoing medical needs, such as weekly therapy sessions or routine check-ups.
Transportation can be requested for various medical needs, as long as the enrollee meets the criteria for the chosen mode of transport. This includes individuals who can walk but require assistance or those who need a stretcher.
While the enrollee’s information is required, a caregiver, family member, or healthcare professional can complete the form on their behalf.
Although this specific form is for New York State Medicaid, similar forms exist in other states. Each state has its own regulations and processes regarding medical transportation.
Approval depends on the review of the submitted information. The Medicaid program evaluates the request based on medical necessity and eligibility criteria.
While preferences can be indicated, the transportation provider must be approved by Medicaid. The program often has a list of authorized providers to ensure compliance and quality of service.
Submitting false information can lead to penalties, including financial restitution. It is crucial that all details provided are accurate and complete.
There may be specific deadlines for submitting the form, especially if transportation is needed for upcoming appointments. It is advisable to submit the request as early as possible.
A physician’s signature is necessary to certify that the requested transportation is medically necessary. This adds an important layer of verification to the process.
Eligibility for different modes of transportation varies based on the enrollee’s medical condition and needs. Each mode has specific requirements that must be met for approval.
Understanding the Medicaid Standing Order form is crucial for ensuring timely and appropriate transportation for medical appointments. Here are some key takeaways:
Filling out the Medicaid Standing Order form accurately can streamline the transportation process, ensuring that patients receive the necessary care without unnecessary delays.