The Medical Application form is an essential document for individuals and families seeking Medi-Cal coverage in California. This form collects vital information about applicants, including personal details, family composition, and income sources. It begins by asking for basic identifying information, such as names, addresses, and contact numbers. Following this, it delves into the specifics of each household member, including their relationship to the primary applicant, gender, marital status, and any disabilities they may have. The form also addresses financial aspects, requiring details about income and expenses, which are crucial for determining eligibility. Additionally, it contains sections that inquire about assets and health coverage, ensuring a comprehensive overview of the applicant's situation. By gathering this information, the form plays a pivotal role in the assessment process for Medi-Cal benefits, helping individuals access the healthcare services they need.
TEAR HERE
State of California - Health and Human ServicesAgency |
Department of Health Care Services |
APPLICATION FOR
To complete this form, use the instructions. Print clearly. Use black or blue ink only.
SECTION 1 Tell us about the person who wants
1 |
|
LAST NAME |
|
FIRST NAME |
|
|
|
|
MIDDLE INITIAL |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
HOMEADDRESS(NUMBERANDSTREET).DO NOT LIST A P.O. BOX UNLESSHOMELESS |
3 |
APARTMENT NUMBER |
|
4 |
HOME PHONE # |
|||||
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
CITY/STATE |
6 |
COUNTY |
|
|
7 |
ZIP CODE |
|
8 |
WORK PHONE # |
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
||
9 |
|
MAILINGADDRESS (IF DIFFERENT FROMABOVE) OR P.O. BOX |
|
|
10 |
APARTMENT NUMBER |
|
11 |
MESSAGE PHONE # |
|||
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
12 |
|
CITY |
|
|
|
|
|
|
|
13 |
ZIP CODE |
|
|
|
|
|
|
|
|
|
|
|
|
||
14A |
WHAT LANGUAGE/DIALECT DO YOU SPEAK BEST? |
|
|
14B |
WHAT LANGUAGE DO YOU READ BEST? |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
TEAR HERE
SECTION 2 Tell us about the person listed in Section 1, his or her family and the children they care for, even if they don’t want coverage.
|
|
Adult 1/Self |
Adult 2 |
Child 1 |
Child 2 |
Child 3 |
|
|
|
|
|
|
|
15 |
Name: |
|
|
|
|
|
|
Last |
|
|
|
|
|
|
|
|
|
|
|
|
First
Middle
16Relationship to person in Section 1.
17If address where living is not the same as listed in Section 1, put address where living:
18 |
Gender: |
❑ Male ❑ Female |
❑ Male ❑ Female |
❑ Male ❑ Female |
❑ Male ❑ Female ❑ Male ❑ Female |
|
|
19 Marital Status: |
❑ Single |
❑ Single |
❑ Single |
❑ Single |
❑ Single |
|
❑ Married |
❑ Married |
❑ Married |
❑ Married |
❑ Married |
|
❑ Divorced |
❑ Divorced |
❑ Divorced |
❑ Divorced |
❑ Divorced |
|
❑ Separated |
❑ Separated |
❑ Separated |
❑ Separated |
❑ Separated |
|
❑ Widowed |
❑ Widowed |
❑ Widowed |
❑ Widowed |
❑ Widowed |
20Name of spouse(s) of married minors in the home.
21 |
Date of Birth: |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
|
|||||||||||
|
|
||||||||||
|
|
MO DAY |
YR |
MO |
DAY YR |
MO |
DAY YR |
MO |
DAY YR |
MO |
DAY YR |
|
|
|
|
|
|
|
|
|
|
|
|
22 |
Pregnant: |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
|
|
Due Date: |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
MO |
DAY |
YR |
MO |
DAY YR |
MO |
DAY YR |
MO |
DAY YR |
MO |
DAY YR |
23 |
Has a physical, mental |
❑Yes ❑ No |
❑Yes ❑ No |
❑Yes ❑ No |
❑Yes ❑ No |
❑Yes ❑ No |
|
or emotional disability? |
|||||
|
|
|
|
|
|
|
|
Disability expected |
❑ 30 Days or More |
❑ 30 Days or More |
❑ 30 Days or More |
❑ 30 Days or More |
❑ 30 Days or More |
|
to last: |
❑12 Months or More |
❑12 Months or More |
❑12 Months or More |
❑12 Months or More |
❑12 Months or More |
|
|
MC 210 2/10 |
A1 |
CONTINUED ➥ |
APPLICATION |
SECTION 2 Continued |
Adult 1/Self |
Adult 2 |
Child 1 |
Child 2 |
Child 3 |
|
24Hasanyoneeverreceived
cash aid, SSI, Food |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
Stamps |
|
|
|
|
|
|
|
|
|
|
If “Yes,” under what name?
25
26 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Wants medical benefits? |
❑ |
Yes |
❑ |
No |
❑ |
Yes |
❑ |
No |
❑ |
Yes |
❑ |
No |
❑ |
Yes |
❑ |
No |
❑ |
Yes |
❑ |
No |
||
|
||||||||||||||||||||||
27Do you own or are
|
|
you buying a home |
|
❑ |
Yes |
❑ |
No |
|
|
❑ |
Yes |
❑ |
No |
|
|
❑ |
Yes |
❑ |
No |
|
❑ |
Yes |
❑ |
No |
❑ |
|
Yes |
❑ |
No |
||||||||||||||
|
|
outside California? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
SECTION 3 |
|
Answer for all children in Section 2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Child 3 |
|
|
|
|
|
|
|
Unborn |
|||||||||||
|
|
|
Child 1 |
|
|
|
|
|
|
Child 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
28 |
|
Mother’s Name: |
|
|
|
|
Mother’s Name: |
|
|
|
|
Mother’s Name: |
|
|
|
|
|
|
|
Mother’s Name: |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Is Mother: |
|
|
|
|
Is Mother: |
|
|
|
|
|
|
Is Mother: |
|
|
|
|
|
|
|
Is Mother: |
|
|
|
|
|
||||||||||||||||||
|
❑ |
Employed |
|
❑ |
Employed |
❑ |
Employed |
|
|
❑ |
Employed |
||||||||||||||||||||||||||||||||
|
❑ |
Disabled |
|
❑ |
Unemployed |
|
|
❑ |
Disabled |
❑ |
Unemployed |
|
❑ |
Disabled |
|
❑ |
Unemployed |
|
❑ |
Disabled |
❑ |
Unemployed |
|||||||||||||||||||||
|
❑ |
Deceased |
|
❑ |
Absent |
|
|
❑ |
Deceased |
❑ |
Absent |
|
❑ |
Deceased |
|
❑ |
Absent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
29 |
|
Father’s Name: |
|
|
|
|
|
Father’s Name: |
|
|
|
|
Father’s Name: |
|
|
|
|
|
|
|
Father’s Name: |
||||||||||||||||||||||
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
Is Father: |
|
❑ |
Employed |
|
Is Father: |
❑ |
Employed |
Is Father: |
|
❑ |
Employed |
|
|
Is Father: |
❑ |
Employed |
|||||||||||||||||||||||||||
|
❑ |
Disabled |
|
❑ |
Unemployed |
|
|
❑ |
Disabled |
❑ |
Unemployed |
|
|
❑ |
Disabled |
|
❑ |
Unemployed |
|
❑ |
Disabled |
❑ |
Unemployed |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❑ |
Deceased |
|
❑ |
Absent |
|
|
❑ |
Deceased |
❑ |
Absent |
|
|
❑ |
Deceased |
|
❑ |
Absent |
|
|
|
❑ |
Deceased |
❑ |
Absent |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION 4 |
List allincome/money received by persons listed in Section 2. |
|||||
|
|
|
|
|
|
|
30 |
|
|
31 |
SOURCE OF INCOME/ |
32 |
HOW MUCH |
|
NAME OF PERSON RECEIVING |
|
MONEY RECEIVED |
|
INCOME/MONEY |
|
|
INCOME/MONEY |
|
|
|||
|
|
(Employment, social security) |
|
IS RECEIVED |
||
|
|
|
|
|
||
|
|
|
|
|
|
|
33HOW OFTEN INCOME/
MONEY RECEIVED
(Monthly, bimonthly, weekly, biweekly, daily)
SECTION 5 Give information about the listed expenses/cost paid by allpersons listed in Section 2.
TYPE OF PAYMENT |
34 |
NAME OF |
35 |
MONTHLY |
YOUR FAMILYMAKES |
PERSON WHO PAYS |
AMOUNT PAID |
||
Child Support
Alimony
Other Health
Insurance Premium
Medicare Premium
36 |
CHILD CARE OR |
37 |
AGE |
38 |
NAME OF |
39 |
MONTHLY |
|
DEPENDENT CARE |
|
|
PERSON WHO PAYS |
AMOUNT PAID |
||
(List child’s or dependent’s name) |
|
|
|||||
|
|
|
|
|
|
||
1.
2.
3.
4.
MC 210 2/10 |
A2 |
APPLICATION |
TEAR HERE
SECTION 6 |
Skip this Section if you are only applying for children under 19 and/or pregnant women |
|
|
|
(pregnancy related services only). |
Otherwise answer for all persons listed in Section 2.
40Does anyone have cash or uncashed checks?
If “Yes,” list amount here |
|
(See instructions) |
41Does anyone have a checking, savings account, or life insurance? (See instructions)
42Is there one car or more in the household? (See instructions)
43Does anyone have a court ordered settlement or judgement? (See instructions)
44Does anyone have
45Does anyone own any items such as stocks, bonds, retirement funds, trusts, real estate, motor vehicles for a business, business accounts, promissory notes, mortgages, deeds of trust, recreational vehicles, burial trusts or funds, annuities, jewelry (not heirloom or wedding), oil or mineral rights? (See instructions)
❑Yes ❑No
❑Yes ❑No
❑Yes ❑No
❑Yes ❑No
❑Yes ❑No
❑Yes ❑No
46 |
Has anyone listed on this form transferred, sold, traded or given away any items such as those |
❑ |
Yes |
❑ |
No |
|
listed above in the last 30 months? (See instructions) |
|
|
|
|
|
|
|
|
|
|
47Have any items listed in this section been spent or used as security for medical costs?
(See instructions) |
❑ |
Yes |
❑ |
No |
TEAR HERE
SECTION 7 |
Answer only for persons who want |
|
|
|
|
|
|
|
|
||
|
Adult 1/Self |
Adult 2 |
Child 1 |
Child 2 |
Child 3 |
48Social Security #:
You may be able to receive
49Place of Birth:
State or Country.
50 |
U.S. Citizen or National? |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
||||||||||
|
If “No,” write in date of |
|
/ |
|
/ |
|
/ |
|
/ |
|
/ |
|
/ |
|
/ |
|
/ |
|
/ |
|
/ |
|
entry into U.S. |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
MO |
DAY |
YR |
MO |
DAY |
YR |
MO |
DAY |
YR |
MO |
DAY |
YR |
MO |
DAY |
YR |
||||||
|
|
||||||||||||||||||||
51Living in a
|
Care or Board and |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
|
Care Facility? |
|
|
|
|
|
|
|
|
|
|
|
If “Yes,” name of |
|
|
|
|
|
|
|
|
|
|
|
facility: |
|
|
|
|
|
|
|
|
|
|
|
Do you intend to |
|
|
|
|
|
|
|
|
|
|
|
return home? |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
|
Do you intend to |
|
|
|
|
|
|
|
|
|
|
|
return home within |
|
|
|
|
|
|
|
|
|
|
|
six months? |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
52 |
Has health/dental or |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
|
vision coverage? |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
53Had medical expenses within the 3 months
|
before the month you |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
|
applied and want Medi- |
|
|
|
|
|
|
|
|
|
|
|
Cal for those expenses. |
|
|
|
|
|
|
|
|
|
|
54 |
Lawsuit pending due |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
❑Yes |
❑ No |
|
to accident or injury? |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
MC 210 2/10 |
A3 |
CONTINUED ➥ |
APPLICATION |
SECTION 7 |
Continued |
|
|
|
|
|
Adult 1/Self |
Adult 2 |
Child 1 |
Child 2 |
Child 3 |
55 |
Current or past |
❑Yes ❑ No |
❑Yes ❑ No |
❑Yes ❑ No |
❑Yes ❑ No |
❑Yes ❑ No |
|
U.S. Military Service |
|||||
|
❑Self |
❑Self |
❑Self |
❑Self |
❑Self |
|
|
for adults, spouse or |
|||||
|
❑Spouse |
❑Spouse |
❑Spouse |
❑Spouse |
❑Spouse |
|
|
child’s parents? |
|||||
|
|
|
|
|
|
|
|
|
❑Parent |
❑Parent |
❑Parent |
❑Parent |
❑Parent |
56 |
Ethnicity (race): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
(optional) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
57 |
In school full time? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❑ |
Yes |
❑ |
No |
❑ |
Yes |
❑ |
No |
❑ |
Yes |
❑ |
No |
❑ |
Yes |
❑ |
No |
❑ |
Yes |
❑ |
No |
|||
|
||||||||||||||||||||||
|
|
58Living away from
home? |
|
❑ |
Yes |
❑ |
No |
❑ |
Yes |
❑ |
No |
❑ |
Yes |
❑ |
No |
❑ |
Yes |
❑ |
No |
❑ |
Yes |
❑ |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION 8 |
Information Release (Optional). |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
59Check this box if you do not want
❑
60
I got help from (give name of person)when I
filled out this application. I agree that the local social services office may give them information about the status of this application. Applicant please initial
SECTION 9 Signature and Certification.
61I declare under penalty of perjury under the laws of the State of California that the answers I have given in this application, and the documents given are correct and true to the best of my knowledge and belief.
I declare that I have read and understand the application instructions, the declarations, and all information printed on this application.
Signature |
|
|
Date |
|
|
|
|
Witness Signature(If person signed with a mark) |
|
|
Date |
|
|
|
|
Signature of person helpingApplicant fill out the form |
Telephone Number |
Relationship toApplicant |
Date |
|
|
|
|
Signature of person acting forApplicant/Beneficiary |
Telephone Number |
Relationship toApplicant |
Date |
For information about any of the following programs, check the box(es) below and
information will be sent to you. Visit our website, www.dhcs.ca.gov
❑ Personal Care Service Program (PCSP).Aprogram for |
❑ Access for Infants, and Mothers (AIM).Aprogram to help pregnant women with moderate income |
obtain health care. |
❑ Woman, Infants and Children Nutrition Program (WIC).Anutrition program for pregnant and |
postpartum women and children under 5. |
❑ Family Planning |
❑ Child Health and Disability Prevention (CHDP) program. Preventive healthcare for children and youth. |
Do you want your children or youth referred to the CHDP program for
❑Yes |
❑No |
MC 210 2/10 |
A4 |
APPLICATION |
| Fact Name | Details |
|---|---|
| Governing Law | California Welfare and Institutions Code, Section 14000 et seq. |
| Purpose of Form | This form is used to apply for Medi-Cal, California's Medicaid program. |
| Eligibility | Eligibility is based on income, family size, and other factors. |
| Required Information | Applicants must provide personal details, income, and household information. |
| Submission Method | The completed form can be submitted online or in person at local social services offices. |
| Language Options | Applicants can indicate their preferred language for communication on the form. |
| Signature Requirement | Applicants must sign and certify the accuracy of the information provided. |
| Confidentiality | Information provided is confidential and used solely for determining eligibility. |
Filling out the Medical Application form requires careful attention to detail. Each section gathers specific information about the applicant and their household. Follow the steps outlined below to ensure that all necessary information is accurately provided.
Once the form is completed, review all entries for accuracy before submission. Ensure that all required signatures are obtained and that the application is submitted to the appropriate office for processing.
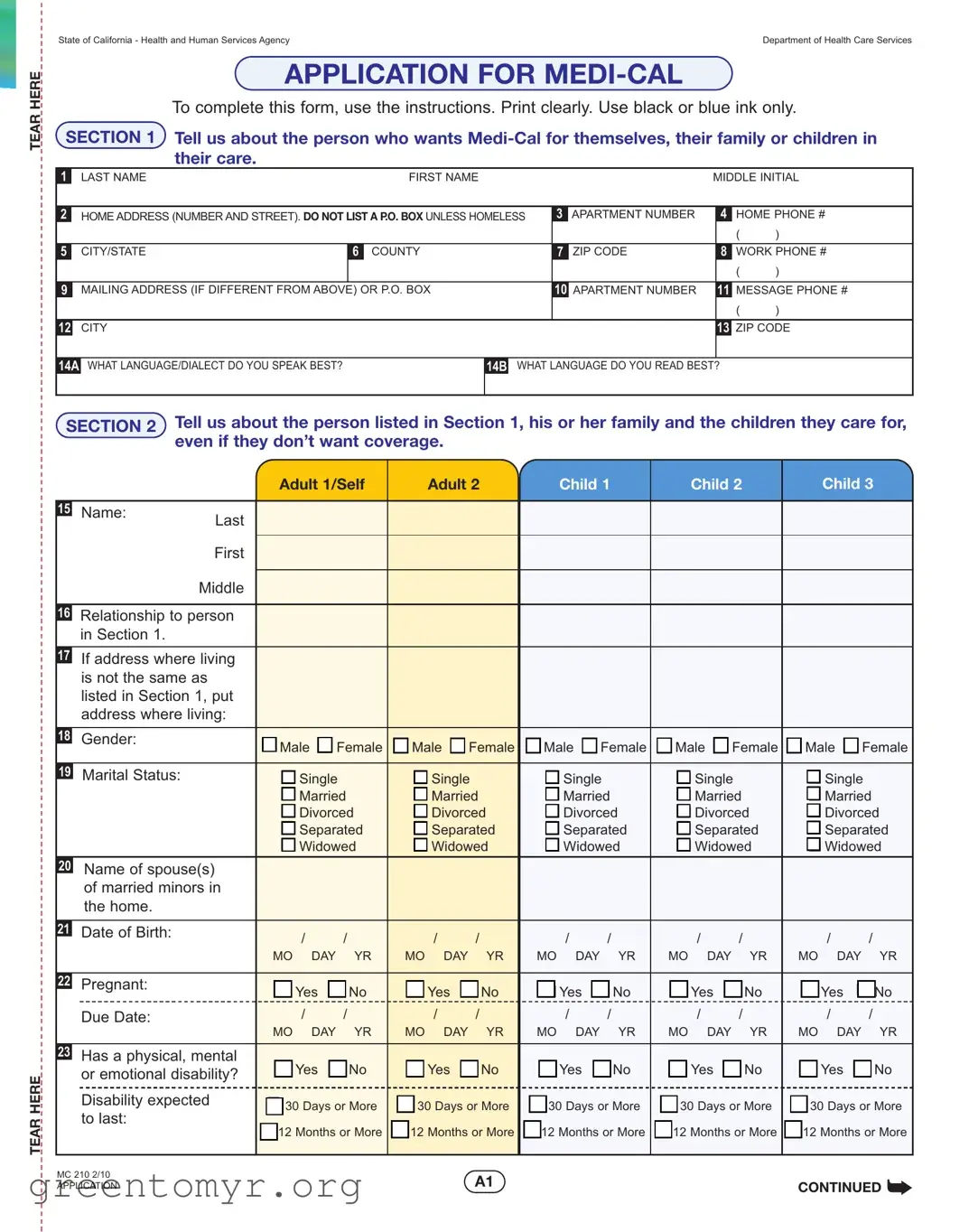
The Medical Application form is designed for individuals and families seeking Medi-Cal coverage in California. It collects essential information about the applicant, their family members, and their financial situation to determine eligibility for health care services.
This form should be completed by anyone applying for Medi-Cal for themselves, their family, or children in their care. It is important to include all relevant family members, even if they do not wish to receive coverage.
In Section 1, you will need to provide personal details about the applicant. This includes:
Section 2 requires information about all family members listed in Section 1. You will need to provide:
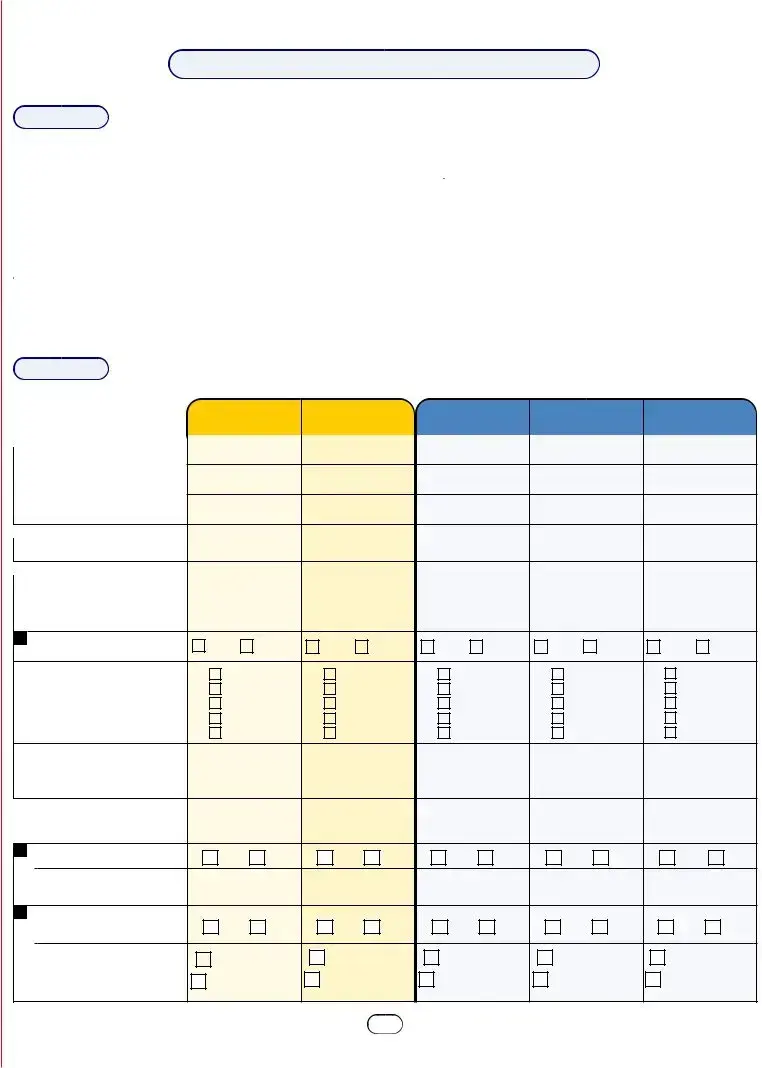
In Section 4, you must list all sources of income for each person included in the application. This includes employment, social security, or any other income. You will also indicate how often this income is received, such as monthly or weekly.
Section 5 asks for details about monthly expenses. You should provide information on payments such as child support, alimony, health insurance premiums, and any other relevant costs. This helps assess your financial situation accurately.
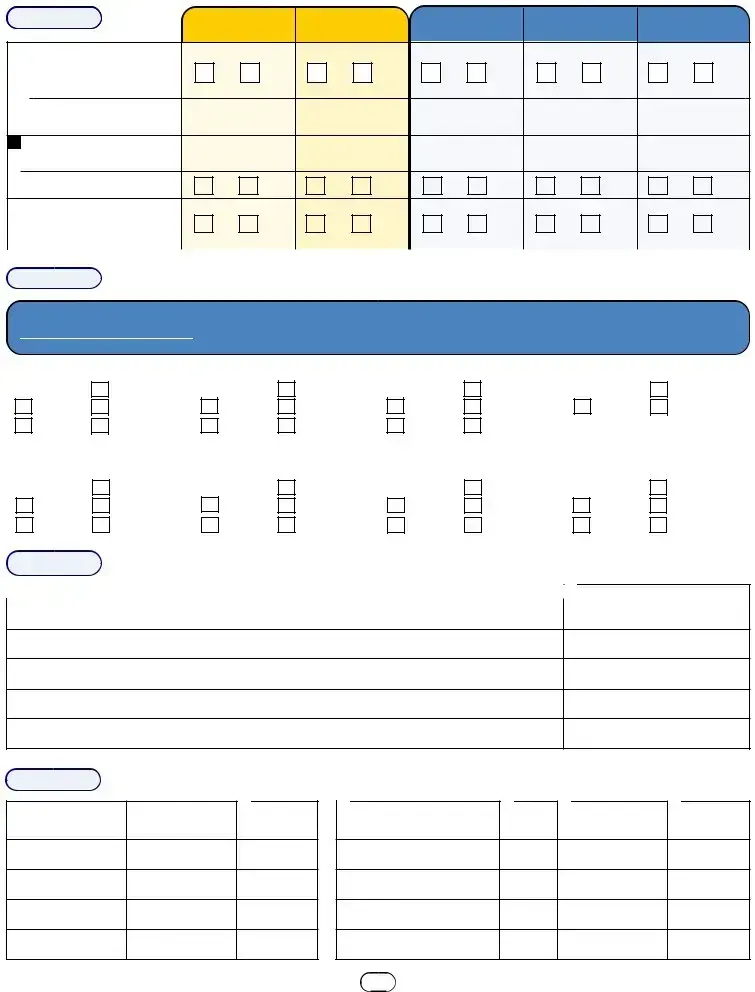
You may still be eligible for Medi-Cal even if you do not possess a Social Security Number. The application allows you to indicate this situation, and additional steps may be provided to assist you in obtaining coverage.
Once the application is submitted, the local social services office will review the information provided. They may contact you for further details or clarification if needed. You will receive notification regarding your eligibility and the next steps in the process.
Filling out the Medical Application form for Medi-Cal can be a daunting task, and mistakes are all too common. Understanding these pitfalls can help ensure a smoother application process. Here are seven frequent mistakes people make when completing the form.
One of the most common errors is illegible handwriting. The application requires clear, printed information. If the handwriting is difficult to read, it could lead to misunderstandings or delays. Using black or blue ink is also crucial, as other colors may not be processed properly.
Another mistake involves incomplete information. Skipping sections or failing to provide necessary details can hinder the application’s progress. Each question is designed to gather specific information, and missing answers can result in delays or even denials of coverage.
Many applicants also forget to include current contact information. Providing accurate home and work phone numbers is essential. If the Medi-Cal office needs to reach you for clarifications or updates, having the correct contact information ensures you won’t miss important communications.
Some people neglect to report all household members. It’s vital to include everyone in the household, even if they do not seek coverage. This oversight can lead to complications in determining eligibility and benefits.
Additionally, failing to answer questions about income sources accurately can create issues. All sources of income should be disclosed, including part-time jobs and assistance programs. Underreporting income may lead to penalties or loss of benefits in the future.
Another frequent error is not signing the application. A signature is a declaration of the truthfulness of the information provided. Without it, the application cannot be processed. Remember, this step is crucial for the form to be considered valid.
Lastly, some applicants overlook the importance of deadlines. Medi-Cal applications must be submitted within specific time frames to ensure timely coverage. Missing a deadline can result in having to reapply, causing unnecessary delays in receiving needed medical care.
By being aware of these common mistakes, applicants can better navigate the Medi-Cal application process. Attention to detail and thoroughness can make a significant difference in securing the health coverage needed.
When applying for Medi-Cal in California, several other forms and documents may be required to complete the application process. These documents help provide a comprehensive view of the applicant's situation and ensure that the application is processed smoothly. Below is a list of commonly used forms and documents that often accompany the Medical Application form.
Gathering these documents in advance can help streamline the application process for Medi-Cal. Each form plays a vital role in ensuring that the application is complete and accurately reflects the applicant's needs and circumstances.
Things to Do:
Things Not to Do:
Misconceptions about the Medical Application form can lead to confusion and delays in obtaining necessary healthcare coverage. Here are eight common misconceptions explained:
Understanding these misconceptions can help applicants navigate the Medi-Cal application process more effectively. It is crucial to seek accurate information and assistance when needed.
When filling out the Medical Application form for Medi-Cal, keep these key takeaways in mind: