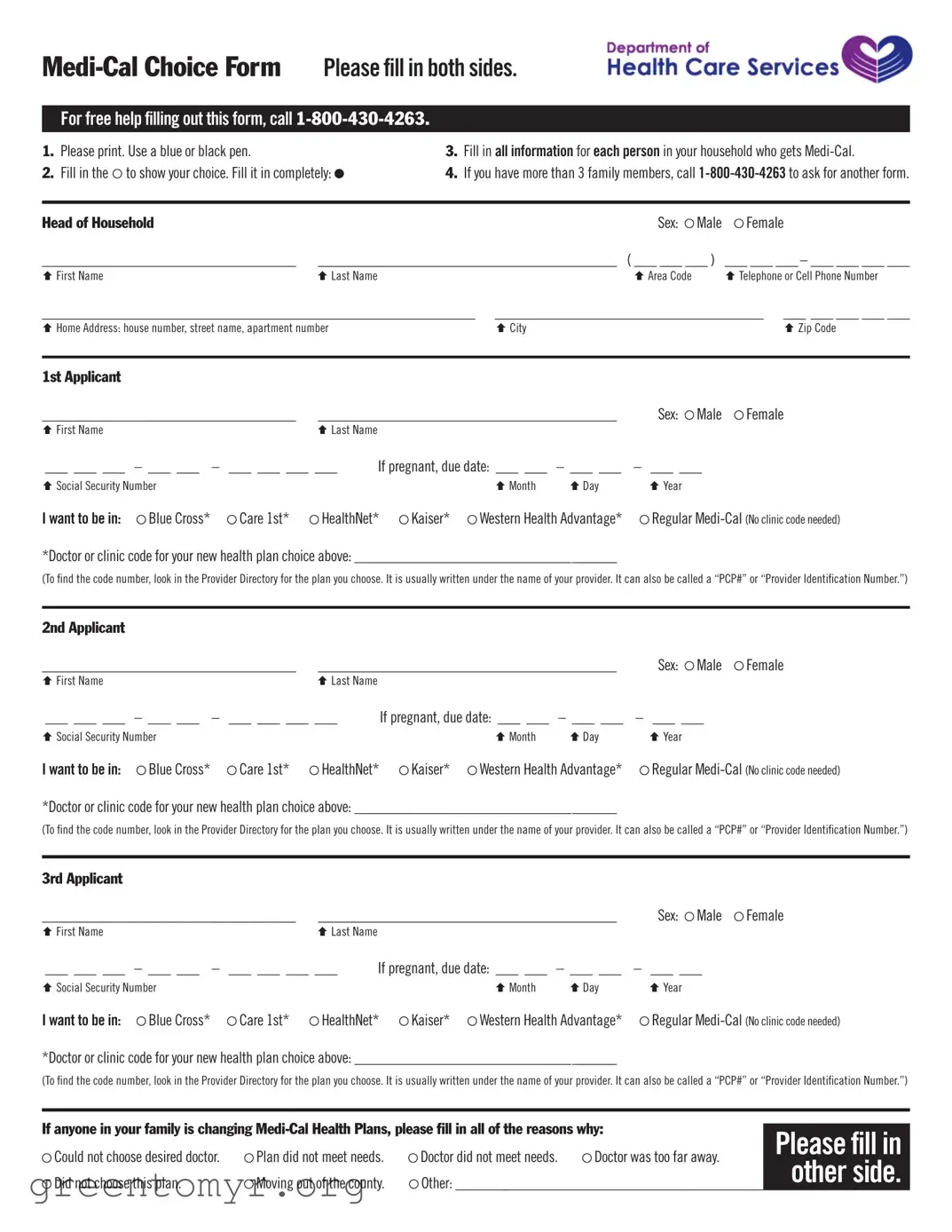
The Medical Choice Form is a vital document for individuals and families enrolled in Medi-Cal, California's Medicaid program. It allows beneficiaries to select their preferred health plan and manage their healthcare needs effectively. The form requires clear and accurate information about each household member receiving Medi-Cal benefits, including personal details such as names, social security numbers, and contact information. Applicants must indicate their health plan choice from options like Blue Cross, HealthNet, Kaiser, and others, while also providing necessary clinic or doctor codes. For those with more than three family members, additional forms can be requested. Importantly, the form includes a statement of understanding, ensuring that applicants are aware of how their information will be used and the implications of their health plan choices. For assistance, individuals can reach out to a dedicated helpline, ensuring that help is readily available for those who need it. Completing the Medical Choice Form accurately is essential for seamless enrollment and access to necessary healthcare services.
For free help filling out this form, call
1. Please print. Use a blue or black pen. |
|
|
3. Fill in all information for each person in your household who gets |
|||||||
2. Fill in the |
to show your choice. Fill it in completely: |
|
4. If you have more than 3 family members, call |
|||||||
|
|
|
|
|
|
|
|
|
|
|
Head of Household |
|
|
|
|
|
|
Sex: |
Male |
Female |
|
__________________________________ |
________________________________________ |
( ___ ___ ___ ) ___ ___ ___ – ___ ___ ___ ___ |
||||||||
Ç First Name |
|
|
Ç Last Name |
|
|
|
|
Ç Area Code |
|
Ç Telephone or Cell Phone Number |
__________________________________________________________ |
____________________________________ ___ ___ ___ ___ ___ |
|||||||||
Ç Home Address: house number, street name, apartment number |
|
|
Ç City |
|
|
|
Ç Zip Code |
|||
|
|
|
|
|
|
|
|
|
|
|
1st Applicant |
|
|
|
|
|
|
|
|
|
|
__________________________________ |
________________________________________ |
Sex: |
Male |
Female |
||||||
Ç First Name |
|
|
Ç Last Name |
|
|
|
|
|
|
|
___ ___ ___ |
– ___ ___ – |
___ ___ ___ ___ |
If pregnant, due date: ___ ___ |
– ___ ___ |
– ___ ___ |
|
||||
Ç Social Security Number |
|
|
|
|
Ç Month |
Ç Day |
Ç Year |
|
|
|
I want to be in: |
Blue Cross* |
Care 1st* |
HealthNet* |
Kaiser* |
Western Health Advantage* |
Regular |
||||
*Doctor or clinic code for your new health plan choice above: ___________________________________ |
|
|
|
|||||||
(To find the code number, look in the Provider Directory for the plan you choose. It is usually written under the name of your provider. It can also be called a “PCP#” or “Provider Identification Number.”)
2nd Applicant |
|
|
|
|
|
|
|
|
__________________________________ |
________________________________________ |
Sex: Male |
Female |
|||||
Ç First Name |
|
|
Ç Last Name |
|
|
|
|
|
___ ___ ___ |
– ___ ___ – |
___ ___ ___ ___ |
If pregnant, due date: ___ ___ |
– ___ ___ |
– ___ ___ |
|
||
Ç Social Security Number |
|
|
|
Ç Month |
Ç Day |
Ç Year |
|
|
I want to be in: |
Blue Cross* |
Care 1st* |
HealthNet* |
Kaiser* |
Western Health Advantage* |
Regular |
||
*Doctor or clinic code for your new health plan choice above: ___________________________________ |
|
|
||||||
(To find the code number, look in the Provider Directory for the plan you choose. It is usually written under the name of your provider. It can also be called a “PCP#” or “Provider Identification Number.”)
3rd Applicant |
|
|
|
|
|
|
|
|
|
__________________________________ |
________________________________________ |
Sex: Male |
Female |
||||||
Ç First Name |
|
|
Ç Last Name |
|
|
|
|
|
|
___ ___ ___ |
– ___ ___ – |
___ ___ ___ ___ |
If pregnant, due date: ___ ___ |
– ___ ___ |
– ___ ___ |
|
|||
Ç Social Security Number |
|
|
|
|
Ç Month |
Ç Day |
Ç Year |
|
|
I want to be in: |
Blue Cross* |
Care 1st* |
HealthNet* |
Kaiser* |
Western Health Advantage* |
Regular |
|||
*Doctor or clinic code for your new health plan choice above: ___________________________________
(To find the code number, look in the Provider Directory for the plan you choose. It is usually written under the name of your provider. It can also be called a “PCP#” or “Provider Identification Number.”)
If anyone in your family is changing |
Please fill in |
||||
Could not choose desired doctor. |
Plan did not meet needs. |
Doctor did not meet needs. |
Doctor was too far away. |
||
other side. |
|||||
Did not choose this plan. |
Moving out of the county. |
|
|
||
Other: ______________________________________________________________ |
|||||
For free help filling out this form, call
STATEMENT OF UNDERSTANDING: I understand that by filling out and signing this form, I am choosing how to get my
I understand that the Department of Health Care Services will keep the information on this form. They will only use it to enroll or disenroll me from a
If You Chose a
If You Join Kaiser: I understand that Kaiser requires binding arbitration. This means that I give up my right to a jury or court trial for medical malpractice and other disagreements about benefits and services. Instead, I would help choose independent professionals who would make a decision about the problem. I can still ask for a
Please Sign Below: |
|
|
|
Head of Household |
__________________________________________ |
Date: ___ ___ – ___ ___ |
– ___ ___ |
|
Ç Signature |
Ç Month Ç Day |
Ç Year |
1st Applicant |
|
if under 18 years, parent or guardian: __________________________________________ |
Date: |
ÇSignature
2nd Applicant |
|
if under 18 years, parent or guardian: __________________________________________ |
Date: |
ÇSignature
3rd Applicant |
|
if under 18 years, parent or guardian: __________________________________________ |
Date: |
ÇSignature
___ ___ – ___ ___ |
– ___ ___ |
|
Ç Month |
Ç Day |
Ç Year |
___ ___ – ___ ___ |
– ___ ___ |
|
Ç Month |
Ç Day |
Ç Year |
___ ___ – ___ ___ |
– ___ ___ |
|
Ç Month |
Ç Day |
Ç Year |
Mail To:
California Dept. of Health Services |
|
|
Health Care Options |
|
|
Box 989009 |
|
|
Please fill in |
||
West Sacramento, CA |
||
other side. |
||
________________________________________________________________________________________________________________ |
| Fact Name | Description |
|---|---|
| Form Purpose | The Medi-Cal Choice Form is used by individuals to select their Medi-Cal health care plan. |
| Eligibility | This form must be completed for each person in a household who receives Medi-Cal benefits. |
| Contact Information | For assistance in filling out the form, individuals can call 1-800-430-4263. |
| Submission Requirements | All information on the form must be printed clearly using a blue or black pen. |
| Family Size | If there are more than three family members, a second form must be requested by calling the provided number. |
| Health Plan Options | Applicants can choose from several health plans, including Blue Cross, HealthNet, and Kaiser. |
| Statement of Understanding | By signing the form, individuals acknowledge their understanding of the enrollment process and their rights regarding their health information. |
| Binding Arbitration | If joining Kaiser, individuals agree to binding arbitration, waiving their right to a jury trial for certain disputes. |
| Mailing Address | The completed form must be mailed to the California Department of Health Services at the specified address in West Sacramento. |
Filling out the Medical Choice form is an essential step in managing your Medi-Cal health care options. Follow these steps carefully to ensure that all required information is accurately provided. If you have any questions or need assistance, you can call 1-800-430-4263 for free help.
The Medical Choice form is a document that allows individuals and families to select their Medi-Cal health plan. This form must be completed for each person in your household who is receiving Medi-Cal benefits. By filling out this form, you indicate your preferred health care provider and plan, ensuring you receive the medical care that best suits your needs.
To fill out the Medical Choice form, follow these steps:
Make sure to double-check your information for accuracy before submitting the form.
If you need assistance while filling out the Medical Choice form, you can call 1-800-430-4263. Trained representatives are available to guide you through the process and answer any questions you may have.
The form requires the following information for each applicant:
Ensure that all information is filled out completely and accurately.
If anyone in your family is changing their Medi-Cal health plan, you will need to provide reasons for the change on the form. Common reasons include:
Make sure to clearly explain your reasons to help facilitate the change.
Once you submit the Medical Choice form, the Department of Health Care Services will process your information. They will use it to enroll or disenroll you from your chosen Medi-Cal health plan. Your information will be kept confidential, but other government agencies that serve Medi-Cal members may access it.
The Statement of Understanding is a section of the form where you acknowledge that you understand the implications of your choices. By signing this statement, you confirm that you are aware of how your information will be used and that you have read the descriptions of the plans available to you.
If you select Kaiser, it is important to note that they require binding arbitration for disputes regarding medical malpractice and other disagreements about benefits and services. This means you will not have the option of a jury or court trial. However, you still have the right to request a Medi-Cal State Hearing if needed.
After completing the Medical Choice form, mail it to:
California Dept. of Health Services
Health Care Options
Box 989009
West Sacramento, CA 95798-9850
Make sure to send it to the correct address to avoid any delays in processing your application.
Filling out the Medical Choice form can be straightforward, but many people make common mistakes that can delay their enrollment or cause confusion. One major error is not printing clearly. The instructions specify that you should use a blue or black pen and print legibly. If the information is hard to read, it may lead to processing issues. Always take your time to ensure that your handwriting is clear and that you follow the instructions closely.
Another frequent mistake involves leaving out required information. Each section of the form asks for specific details about all household members receiving Medi-Cal. If you skip any fields, such as the Social Security number or the health plan choice, it could result in delays. Make sure to double-check that every box is filled out completely before submitting the form.
People often forget to indicate their health plan choice. This is a crucial part of the form. If you do not select a plan, the Department of Health Care Services cannot process your application. Make sure to fill in the plan you want and include the doctor or clinic code if applicable. If you're unsure about the code, refer to the Provider Directory as instructed.
Some applicants also overlook the need to sign the form. A signature is essential to validate your choices and confirm your understanding of the terms. Without it, the form is incomplete. Remember, if you are signing on behalf of a minor, a parent or guardian's signature is required for each applicant under 18.
Lastly, many people fail to mail the form to the correct address. The form must be sent to the California Department of Health Services at the specified address. Ensure that you have the correct mailing information and consider using a method that allows you to track the delivery. Taking these steps can help ensure that your application is processed smoothly and without unnecessary delays.
When navigating the Medi-Cal system, you may encounter various forms and documents that work in tandem with the Medical Choice form. Understanding these documents can help ensure that you receive the care and benefits you need. Below is a list of common forms that you may need to complete or refer to as part of your Medi-Cal journey.
Understanding these documents can empower you to navigate the Medi-Cal system more effectively. Each form serves a unique purpose, and being familiar with them can help ensure that you and your family receive the healthcare services you need without unnecessary delays. If you have questions about any of these forms, don't hesitate to reach out for assistance.
The Medical Choice form is similar to several other documents that serve related purposes in healthcare enrollment and decision-making. Below is a list of these documents and their similarities:
When filling out the Medical Choice form, there are several important guidelines to follow. Adhering to these recommendations can help ensure that your application is processed smoothly.
Conversely, there are also actions to avoid when completing this form:
Misconceptions about the Medical Choice form can lead to confusion and errors in the enrollment process. Here are seven common misconceptions explained:
Filling out the Medical Choice form is a crucial step for families seeking Medi-Cal health coverage. Here are some key takeaways to ensure a smooth experience:
By keeping these points in mind, families can navigate the Medical Choice form with greater confidence and ease.