The Medicare Annual Wellness Visit form serves as an essential tool for seniors to communicate their health status and needs during their annual check-up. This form prompts patients to provide key information, starting with basic demographics such as age and gender. It delves into emotional and physical well-being by asking about feelings of anxiety, depression, and social limitations experienced in the past month. Questions regarding pain levels, support systems, and the ability to perform daily activities—like shopping, meal preparation, and personal care—help healthcare providers assess a patient’s overall health and independence. Additionally, the form addresses lifestyle factors, including exercise habits, alcohol consumption, and medication adherence. Understanding these aspects allows doctors to tailor their care plans effectively. Completing this form before the visit ensures that discussions during the appointment are focused and productive, ultimately leading to better health outcomes for Medicare beneficiaries.
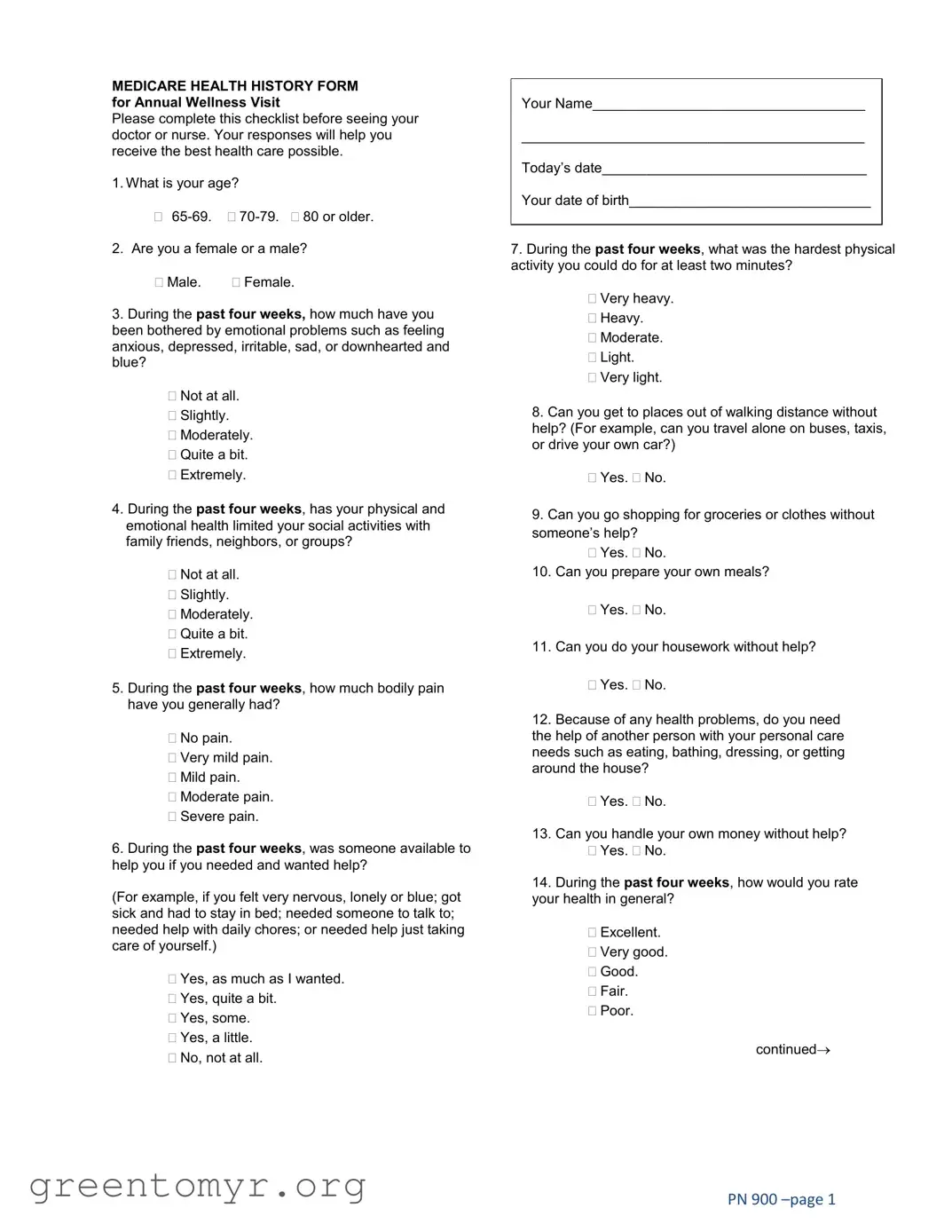
MEDICARE HEALTH HISTORY FORM for Annual Wellness Visit
Please complete this checklist before seeing your doctor or nurse. Your responses will help you receive the best health care possible.
1.What is your age?
2.Are you a female or a male?
Male. Female.
3.During the past four weeks, how much have you been bothered by emotional problems such as feeling anxious, depressed, irritable, sad, or downhearted and blue?
Not at all.
Slightly.
Moderately.
Quite a bit.
Extremely.
4.During the past four weeks, has your physical and emotional health limited your social activities with family friends, neighbors, or groups?
Not at all.
Slightly.
Moderately.
Quite a bit.
Extremely.
5.During the past four weeks, how much bodily pain have you generally had?
No pain.
Very mild pain.
Mild pain.
Moderate pain.
Severe pain.
6.During the past four weeks, was someone available to help you if you needed and wanted help?
(For example, if you felt very nervous, lonely or blue; got sick and had to stay in bed; needed someone to talk to; needed help with daily chores; or needed help just taking care of yourself.)
Yes, as much as I wanted.
Yes, quite a bit.
Yes, some.
Yes, a little.
No, not at all.
Your Name___________________________________
____________________________________________
Today’s date__________________________________
Your date of birth_______________________________
7.During the past four weeks, what was the hardest physical activity you could do for at least two minutes?
Very heavy.
Heavy.
Moderate.
Light.
Very light.
8.Can you get to places out of walking distance without help? (For example, can you travel alone on buses, taxis, or drive your own car?)
Yes. No.
9.Can you go shopping for groceries or clothes without someone’s help?
Yes. No.
10.Can you prepare your own meals?
Yes. No.
11.Can you do your housework without help?
Yes. No.
12.Because of any health problems, do you need
the help of another person with your personal care needs such as eating, bathing, dressing, or getting around the house?
Yes. No.
13.Can you handle your own money without help?
Yes. No.
14.During the past four weeks, how would you rate your health in general?
Excellent.
Very good.
Good.
Fair.
Poor.
continued→
PN 900
Patient Name_______________________________________ DOB____________________Today’s Date_________________
15.How have things been going for you during the past four weeks?
Very well; could hardly be better.
Pretty well.
Good and bad parts about equal.
Pretty bad.
Very bad; could hardly be worse.
16.Are you having difficulties driving your car?
Yes, often.
Sometimes.
No.
Not applicable, I do not use a car.
17.Do you always fasten your seat belt when you are in a car?
Yes, usually.
Yes, sometimes.
No.
18.How often during the past four weeks have you been BOTHERED by any of the following problems?
|
Never |
Seldom |
Sometime |
Often |
Always |
|
|
|
|
|
|
Falling or dizzy when standing up |
|
|
|
|
|
Sexual problems |
|
|
|
|
|
Trouble eating well |
|
|
|
|
|
Teeth or denture problems |
|
|
|
|
|
Problems using the telephone |
|
|
|
|
|
Tiredness or fatigue |
|
|
|
|
|
19.Have you fallen two or more times in the past year?
Yes. No.
20.Are you afraid of falling?
Yes. No.
21.Are you a smoker?
No.
Yes, and I might quit.
Yes, but I’m not ready to quit.
Checklist to bring to your appointment:
22.During the past four weeks, how many drinks of wine, beer, or other alcoholic beverages did you have?
10 or more drinks per week.
One drink or less per week.
No alcohol at all.
23.Do you exercise for about 20 minutes three or more days a week?
Yes, most of the time. Yes, some of the time.
No, I usually do not exercise this much.
24.Have you been given any information to help you with the following:
Hazards in your house that might hurt you?
Yes. No.
Keeping track of your medications?
Yes. No.
25.How often do you have trouble taking medicines the way you have been told to take them?
I do not have to take medicine.
I always take them as prescribed.
Sometimes I take them as prescribed.
I seldom take them as prescribed.
26.How confident are you that you can control and manage most of your health problems?
Very confident.
Somewhat confident.
Not very confident.
I do not have any health problems.
27.What is your race? (Check all that apply.)
White.
Black or African American.
Asian.
Native Hawaiian or Other Pacific Islander.
American Indian or Alaskan Native.
Hispanic or Latino origin or descent.
Other.
Thank you very much for completing your Medicare Health History. Please give the completed form to your doctor or nurse.
PN 900
| Fact Name | Details |
|---|---|
| Purpose | The Medicare Annual Wellness Visit form helps assess a patient's health status and needs. |
| Eligibility | Medicare beneficiaries who have had Part B for at least 12 months can use this form. |
| Health History | The form includes questions about emotional well-being, physical health, and social activities. |
| Checklist Requirement | Patients are advised to bring medical records and a list of medications to their appointment. |
| Frequency | The Annual Wellness Visit can be conducted once every 12 months. |
| State-Specific Forms | Some states may have specific requirements; for example, California follows the California Welfare and Institutions Code. |
| Confidentiality | All information provided on the form is confidential and used for healthcare purposes only. |
| Rating Health | Patients rate their general health on a scale from excellent to poor. |
| Exercise Inquiry | The form asks about exercise habits to promote physical activity among seniors. |
| Fall Risk Assessment | Questions about falls help identify patients at risk for future falls and injuries. |
Completing the Medicare Annual Wellness Visit form is an important step in preparing for your appointment. This form gathers essential information about your health history and current status, which helps healthcare providers deliver personalized care. Follow these steps to fill out the form accurately.
The Medicare Annual Wellness Visit form is designed to gather important health information about you before your appointment. By completing this form, you help your healthcare provider understand your health status, any emotional challenges you may be facing, and how these factors may affect your daily activities. This information allows for a more personalized and effective healthcare plan tailored to your specific needs.
When attending your Annual Wellness Visit, it is essential to bring several key items to ensure a productive appointment. Consider the following checklist:
Having these documents readily available can facilitate a comprehensive discussion about your health with your provider.
The form includes specific questions aimed at assessing both emotional and physical well-being. For instance, it asks about feelings of anxiety, depression, and how these emotional states may limit social activities. Similarly, it inquires about physical pain levels and the ability to perform daily tasks independently. This dual focus helps healthcare providers identify areas where you may need support, enabling them to recommend appropriate resources or interventions.
Once you have filled out the Medicare Annual Wellness Visit form, you should present it to your doctor or nurse at the beginning of your appointment. Your healthcare provider will review your responses and use the information to guide the discussion during your visit. This process ensures that your healthcare team is well-informed about your current health status and can make tailored recommendations based on your individual circumstances.
Completing the Medicare Annual Wellness Visit form is an important step in receiving quality health care. However, there are common mistakes that individuals often make when filling out this form. Recognizing these errors can help ensure that your health care provider has the necessary information to assist you effectively.
One frequent mistake is not providing accurate demographic information. For example, failing to correctly indicate your age or gender can lead to miscommunication and inappropriate care recommendations. It is crucial to double-check these details to ensure they reflect your current status.
Another common error involves the emotional health section. Many individuals may underestimate their feelings, such as anxiety or depression, by selecting “not at all” or “slightly” when they may actually be experiencing more significant issues. Being honest about your emotional state is vital, as it helps your healthcare provider understand your needs better.
People often overlook the importance of the social activity questions. Responding inaccurately about limitations in social interactions can lead to missed opportunities for support and intervention. If you feel that your health has affected your ability to engage with family or friends, it is essential to communicate this clearly.
Additionally, some individuals may not fully consider their physical limitations when answering questions about daily activities. For instance, stating that you can prepare your own meals or handle personal care without help, when in reality you struggle, can hinder the assistance you may need. It is important to reflect on your capabilities honestly.
Lastly, many people forget to bring the necessary documents to their appointment. This includes medical records and lists of medications. Failing to provide this information can delay your care or result in less informed decisions by your healthcare provider. Always remember to prepare these items ahead of time to ensure a productive visit.
The Medicare Annual Wellness Visit is an important step in maintaining your health. To ensure a comprehensive evaluation, several other forms and documents are often used in conjunction with this visit. Below is a list of common documents that may be required or helpful during your appointment.
Having these documents prepared and organized can significantly enhance the effectiveness of your Medicare Annual Wellness Visit. It ensures that healthcare providers have all the necessary information to offer you the best possible care.
The Medicare Annual Wellness Visit form is essential for gathering comprehensive health information from patients. Several other documents share similarities with this form in terms of purpose and content. Below is a list of nine documents that are comparable to the Medicare Annual Wellness Visit form, each serving a unique role in patient care.
Each of these documents plays a vital role in ensuring that healthcare providers have a thorough understanding of a patient's health status, needs, and preferences, ultimately leading to more personalized and effective care.
When filling out the Medicare Annual Wellness Visit form, careful attention can enhance the accuracy of your responses. Below are five key things to do and avoid during this process.
Understanding the Medicare Annual Wellness Visit form is crucial for seniors seeking to optimize their healthcare experience. However, several misconceptions often arise regarding this important document. Below are some of these misconceptions, along with clarifications to help alleviate any concerns.
By addressing these misconceptions, seniors can approach their Medicare Annual Wellness Visit with greater confidence and understanding. This proactive step can lead to improved health outcomes and a more tailored healthcare experience.
Completing the Medicare Annual Wellness Visit form is an important step in ensuring you receive comprehensive health care. Here are some key takeaways to keep in mind:
By keeping these points in mind, you can help ensure that your Annual Wellness Visit is as beneficial as possible.