Understanding the Medicare Part B Redetermination form is crucial for anyone navigating the complexities of Medicare claims. This form serves as a key tool for appealing decisions made on claims, allowing providers and beneficiaries to contest determinations that they believe are incorrect. Each section of the form must be meticulously filled out to avoid dismissal of the request. Important details such as the provider's name, address, and the beneficiary's Medicare number must be provided in uppercase letters. Additionally, it is essential to submit the request within 120 days of the original claim determination. The form also includes specific instructions for various scenarios, such as those involving overpayment decisions or Medicare Secondary Payer situations. Attachments like remittance advice notices and relevant medical documentation are necessary to support your appeal. Failure to use the form correctly could lead to complications, so it's vital to follow the guidelines closely. Understanding these requirements can significantly impact the outcome of your appeal.
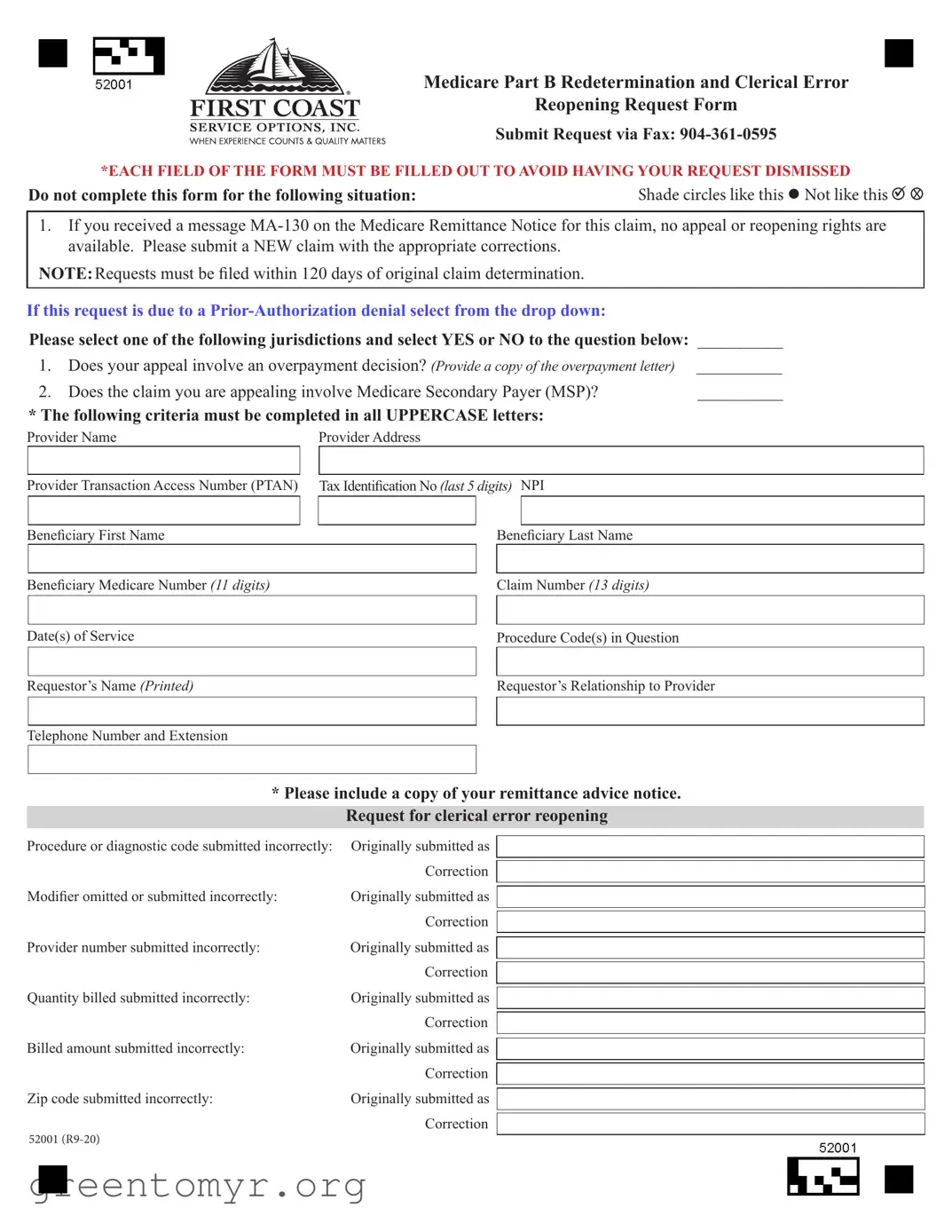
Medicare Part B Redetermination and Clerical Error
Reopening Request Form
Submit Request via Fax:
*EACH FIELD OF THE FORM MUST BE FILLED OUT TO AVOID HAVING YOUR REQUEST DISMISSED
Do not complete this form for the following situation: |
Shade circles like this Not like this |
|
X |
1.If you received a message
NOTE:Requests must be filed within 120 days of original claim determination.
If this request is due to a
Please select one of the following jurisdictions and select YES or NO to the question below: __________
1. |
Does your appeal involve an overpayment decision? (Provide a copy of the overpayment letter) |
__________ |
||
2. |
Does the claim you are appealing involve Medicare Secondary Payer (MSP)? |
__________ |
||
* The following criteria must be completed in all UPPERCASE letters: |
|
|||
Provider Name |
Provider Address |
|
||
|
|
|
|
|
Provider Transaction Access Number (PTAN) |
|
Tax Identification No (last 5 digits) NPI |
|
|
Beneficiary First Name
Beneficiary Last Name
|
|
|
Beneficiary Medicare Number (11 digits) |
|
Claim Number (13 digits) |
|
|
|
Date(s) of Service
Procedure Code(s) in Question
Requestor’s Name (Printed)
Requestor’s Relationship to Provider
Telephone Number and Extension
*Please include a copy of your remittance advice notice. Request for clerical error reopening
Procedure or diagnostic code submitted incorrectly: |
Originally submitted as |
|
Correction |
Modifier omitted or submitted incorrectly: |
Originally submitted as |
|
Correction |
Provider number submitted incorrectly: |
Originally submitted as |
|
Correction |
Quantity billed submitted incorrectly: |
Originally submitted as |
|
Correction |
Billed amount submitted incorrectly: |
Originally submitted as |
|
Correction |
Zip code submitted incorrectly: |
Originally submitted as |
52001 |
Correction |
|
Redetermination request: Dissatisfaction with the original claim determination
The reason I disagree with the initial determination is:
This is an appeal of an overpayment request
The service was medically necessary
The service was denied as a duplicate incorrectly
The service was not overutilized
The service was denied indicating there was other insurance involvement
Additional narrative:
Please attach all pertinent documentation
q Ambulance run sheet |
q History and physical |
q Invoices for unlisted procedures and medication |
q Diagnostic test results |
q Pathology reports |
q Progress notes |
q Other medical records |
|
Improper use of this form and additional guidance
Telephone reopenings can be requested using our interactive voice response system (IVR) at
Unprocessable claims denied with remittance advice message MA130 may not be appealed. Please correct the claim and resubmit.
If the service at issue has already received a redetermination decision, do not use this form. Please use the reconsideration request form located at https://medicare.fcso.com/Forms/138073.pdf.
Appeals for durable medical equipment services (DME) must be appealed to the appropriate DME Medicare administrative contractor
Overpayments resulting from billing errors or MSP/Other Payer Involvement should be reported using the overpayment refund form located at https://medicare.fcso.com/Forms/138379.pdf.
NOTICE - Anyone who misrepresents or falsifies essential information requested by this
form may upon conviction be subject to fine and imprisonment under federal Law.
PrintReset
medicare.fcso.com
First Coast Service Options Inc.
52001
| Fact Name | Details |
|---|---|
| Submission Method | The Medicare Part B Redetermination form can be submitted via fax at 904-361-0595. |
| Mandatory Fields | Every field on the form must be filled out completely to prevent dismissal of the request. |
| Timeframe for Requests | Requests must be filed within 120 days of the original claim determination. |
| Overpayment Decision | If the appeal involves an overpayment decision, a copy of the overpayment letter must be provided. |
| Uppercase Requirement | All required information, such as provider and beneficiary details, must be completed in uppercase letters. |
| Clerical Error Reopening | The form can be used for clerical error reopening requests, detailing the specific correction needed. |
| Improper Use Warning | Misuse of this form can lead to legal consequences, including fines and imprisonment under federal law. |
| Additional Resources | For claims involving durable medical equipment, a different form must be used, and overpayment issues have their own specific forms. |
After filling out the Medicare Part B Redetermination form, the next step involves submitting it correctly to ensure your request is processed. Be sure to provide all necessary documentation and check that every field is completed accurately. Incomplete forms may lead to dismissal of your request.
The Medicare Part B Redetermination form is used to request a review of a claim determination made by Medicare. This form is appropriate for individuals or providers who disagree with the initial decision regarding coverage or payment for services rendered. It allows for an opportunity to present additional information or correct errors related to the claim.
The completed Medicare Part B Redetermination form must be submitted via fax to 904-361-0595. It is important to ensure that every field on the form is filled out completely to avoid dismissal of the request. Incomplete forms may lead to delays or rejection of the appeal.
All required fields must be completed in uppercase letters. Essential information includes:
Additionally, a copy of the remittance advice notice should be included with the submission.
This form should not be used for claims that received a message MA-130 on the Medicare Remittance Notice. For these situations, a new claim must be submitted with the necessary corrections. Furthermore, if a redetermination decision has already been made for the service in question, the reconsideration request form should be used instead.
Requests for redetermination must be filed within 120 days of the original claim determination. It is crucial to adhere to this time frame to ensure that the appeal is considered.
Any individual who misrepresents or falsifies information on the Medicare Part B Redetermination form may face serious consequences. Upon conviction, this can lead to fines and imprisonment under federal law. Accuracy and honesty in completing the form are imperative.
Filling out the Medicare Part B Redetermination form can be a straightforward process, but many people make common mistakes that can lead to delays or outright dismissal of their requests. One major mistake is not filling out every field of the form. Each section must be completed to avoid having the request dismissed. Leaving any field blank can cause unnecessary complications.
Another frequent error is using lowercase letters instead of uppercase. The instructions clearly state that certain fields, such as the provider's name and beneficiary's Medicare number, must be filled out in uppercase letters. Ignoring this requirement can result in processing delays.
Many individuals also fail to provide the necessary documentation. The form requests specific documents, such as a copy of the remittance advice notice. Not including these documents can lead to a rejection of the request. It's crucial to double-check that all required paperwork is attached before submission.
Some people mistakenly use the wrong form for their situation. For example, if a service has already received a redetermination decision, the correct form is the reconsideration request form, not the redetermination form. Using the wrong form can result in a complete halt to the appeal process.
Another common mistake involves not providing a clear reason for the appeal. The section asking for the reason for disagreement must be filled out with specific details. Vague or incomplete explanations can lead to confusion and may result in the request being dismissed.
Additionally, individuals often overlook the requirement to submit requests within the specified time frame. Requests must be filed within 120 days of the original claim determination. Missing this deadline can mean losing the right to appeal entirely.
Improperly shading the circles on the form is another mistake that can lead to complications. The instructions specify how to mark the circles correctly. Failure to follow these guidelines can create confusion in processing the request.
Lastly, individuals sometimes neglect to check for clerical errors before submission. Simple mistakes, such as incorrect procedure codes or billing amounts, can derail the appeal process. Taking a moment to review the information for accuracy can save time and frustration later on.
When navigating the Medicare Part B Redetermination process, it's essential to have the right forms and documents ready. Below is a list of other forms and documents that are often used in conjunction with the Redetermination form. Each plays a vital role in ensuring your appeal is processed smoothly and efficiently.
Having these documents prepared can significantly improve your chances of a successful appeal. Make sure to review each document carefully and submit them alongside your Medicare Part B Redetermination form to avoid any delays in processing your request.
The Medicare Part B Redetermination form serves a specific purpose in the appeals process for Medicare claims. However, it shares similarities with several other important documents in the healthcare and insurance landscape. Here’s a look at six documents that are similar to the Medicare Part B Redetermination form, along with a brief explanation of how they relate to it:
Each of these documents plays a crucial role in ensuring that providers and beneficiaries can effectively navigate the complexities of Medicare claims and appeals. Understanding their similarities can help streamline the process and ensure that all necessary information is provided in a timely manner.
When filling out the Medicare Part B Redetermination form, it is essential to follow specific guidelines to ensure your request is processed correctly. Below is a list of things you should and shouldn't do.
By adhering to these guidelines, you can improve the chances of your redetermination request being accepted and processed efficiently.
Understanding the Medicare Part B Redetermination form can be challenging. Here are five common misconceptions that may lead to confusion:
This is not true. The Redetermination form is specifically for appealing decisions related to Medicare Part B claims. If the claim was denied with the remittance advice message MA-130, a new claim must be submitted instead.
In fact, every field of the form must be filled out completely. Incomplete forms may result in the dismissal of the request, which can delay the resolution of the issue.
This is incorrect. Requests for redetermination must be filed within 120 days of the original claim determination. Missing this deadline means losing the right to appeal.
While the form can address certain clerical errors, it is important to understand the specific types of errors that qualify. Errors such as incorrect procedure codes or provider numbers can be corrected, but not all mistakes are eligible for this form.
This is a misunderstanding. If a claim has already received a redetermination decision, a different form, the reconsideration request form, must be used. It is crucial to select the correct form to avoid unnecessary delays.
When filling out the Medicare Part B Redetermination form, it is crucial to understand the following key points:
Understanding these points can help ensure that your appeal process is smooth and effective.