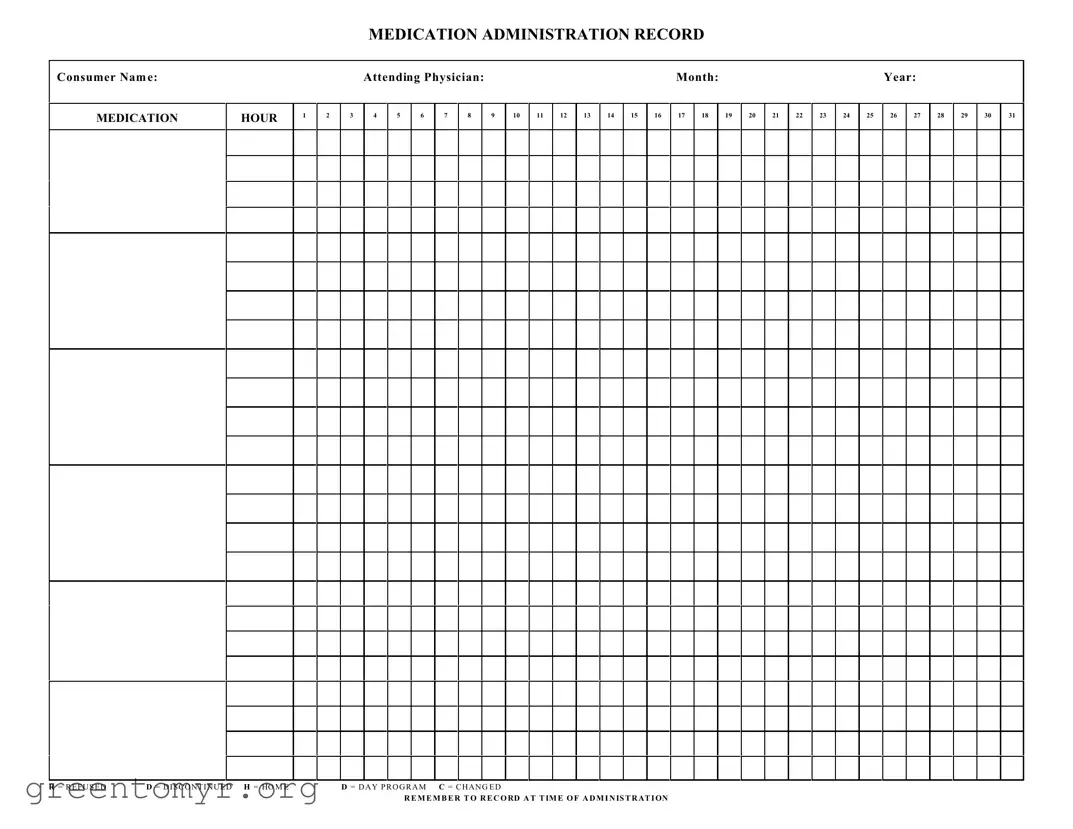
The Medication Administration Record Sheet is an essential tool used in healthcare settings to ensure accurate tracking of medication administration for patients. This form captures vital information, including the consumer's name, the attending physician, and the specific month and year of treatment. It provides a structured way to document the administration of medications throughout the day, with designated hours for each entry. The form includes codes for various situations, such as refusing medication, discontinuing a medication, or changes in the treatment plan, ensuring clarity in communication among healthcare providers. Additionally, the sheet emphasizes the importance of recording medication administration at the exact time it occurs, which is crucial for maintaining patient safety and effective care. By utilizing this form, healthcare professionals can enhance accountability and streamline the medication management process, ultimately contributing to better patient outcomes.
MEDICATION ADMINISTRATION RECORD
Consumer Nam e:
MEDICATION
HOUR
1
2
|
Attending Physician: |
|
|
|
|
|
|
|
|
Month: |
|
|
|
|
|
|
|
Year: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
5 |
6 |
7 |
8 |
|
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
|
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
29 |
30 |
31 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R = R E F U S E D |
D = D I S C O N T I N U E D H = HO M E |
D = D A Y P R O G R A M C = C H A N G E D |
R E M E M B E R T O R E C O RD A T T IM E O F A D M I N IS T R AT I ON
| Fact Name | Details |
|---|---|
| Purpose | The Medication Administration Record (MAR) is used to document the administration of medications to consumers. |
| Consumer Identification | Each MAR must include the consumer's name for accurate tracking of medication administration. |
| Physician's Role | The attending physician's name is required to ensure accountability and proper oversight. |
| Monthly Tracking | The form allows for daily medication tracking throughout the month, covering all 31 days. |
| Administration Hours | Medications can be documented for specific hours, allowing for precise timing of administration. |
| Refusal and Discontinuation Codes | Standard codes (R, D, H, C) are used to indicate if a medication was refused, discontinued, or changed. |
| State-Specific Regulations | Each state may have specific laws governing the use of MARs, such as the California Code of Regulations Title 22. |
| Documentation Requirement | It is essential to record the administration at the time it occurs to maintain accurate medical records. |
| Day Program Indication | The MAR includes a section to indicate if medications are administered during a day program. |
| Compliance Importance | Proper use of the MAR is critical for compliance with healthcare regulations and ensuring consumer safety. |
Once you have the Medication Administration Record Sheet in front of you, it’s time to fill it out accurately. This form plays a crucial role in tracking medication administration for consumers. Each section requires careful attention to ensure that all necessary information is recorded correctly.
The Medication Administration Record Sheet (MARS) is designed to document the administration of medications to individuals. It serves as a critical tool for healthcare providers to track what medications have been given, when they were administered, and any refusals or changes in medication. Accurate records help ensure patient safety and compliance with treatment plans.
When completing the MARS, follow these steps:
If a consumer refuses a medication, mark the corresponding date and hour with an "R" on the MARS. For discontinued medications, use a "D" in the same way. Additionally, note any relevant details about the refusal or discontinuation in the comments section, if available. This information can be crucial for ongoing treatment decisions.
Recording medication changes is vital for several reasons:
Always use "C" to indicate a change and document the new medication details as soon as possible.
One common mistake when filling out the Medication Administration Record Sheet is neglecting to include the consumer's name. This oversight can lead to confusion, especially in facilities where multiple patients receive medication. Accurate identification is crucial for ensuring that the right individual receives the correct dosage. Always double-check that the name is clearly written at the top of the form.
Another frequent error is failing to document the time of administration. It is essential to record the exact time when medication is given. This information helps healthcare providers monitor the effectiveness of the medication and ensures compliance with prescribed schedules. Without this detail, it becomes challenging to track medication adherence and potential side effects.
Some individuals mistakenly use incorrect codes when indicating the status of medication. For example, using "D" for discontinued medication without confirming that it has indeed been stopped can lead to serious health risks. Each code, such as "R" for refused or "H" for home, carries specific implications. Understanding and applying these codes accurately is vital for maintaining proper records.
Lastly, a common oversight is failing to update the attending physician's name or the date. If these details are incorrect or missing, it can create complications in communication and treatment plans. Keeping this information current ensures that all team members are on the same page and can provide the best care possible.
The Medication Administration Record (MAR) Sheet is a vital document used in healthcare settings to track the administration of medications to patients. Alongside the MAR, several other forms and documents play crucial roles in ensuring proper medication management and patient care. Here is a list of related documents that are often utilized in conjunction with the MAR.
In summary, these documents work together with the Medication Administration Record Sheet to create a comprehensive system for medication management. Their proper use enhances patient safety, promotes effective communication among healthcare providers, and ensures that patients receive the best possible care.
The Medication Administration Record Sheet (MARS) is an important document in healthcare settings. It shares similarities with several other forms used in medication management and patient care. Below are six documents that have comparable functions or purposes:
When filling out the Medication Administration Record Sheet form, it is important to follow specific guidelines to ensure accuracy and compliance. Below is a list of things to do and avoid.
Understanding the Medication Administration Record Sheet (MARS) is crucial for effective medication management. However, several misconceptions can lead to confusion. Here are seven common misunderstandings:
Being aware of these misconceptions can help ensure proper use of the Medication Administration Record Sheet, ultimately enhancing patient care and safety.
When filling out and using the Medication Administration Record Sheet form, keep these key takeaways in mind: