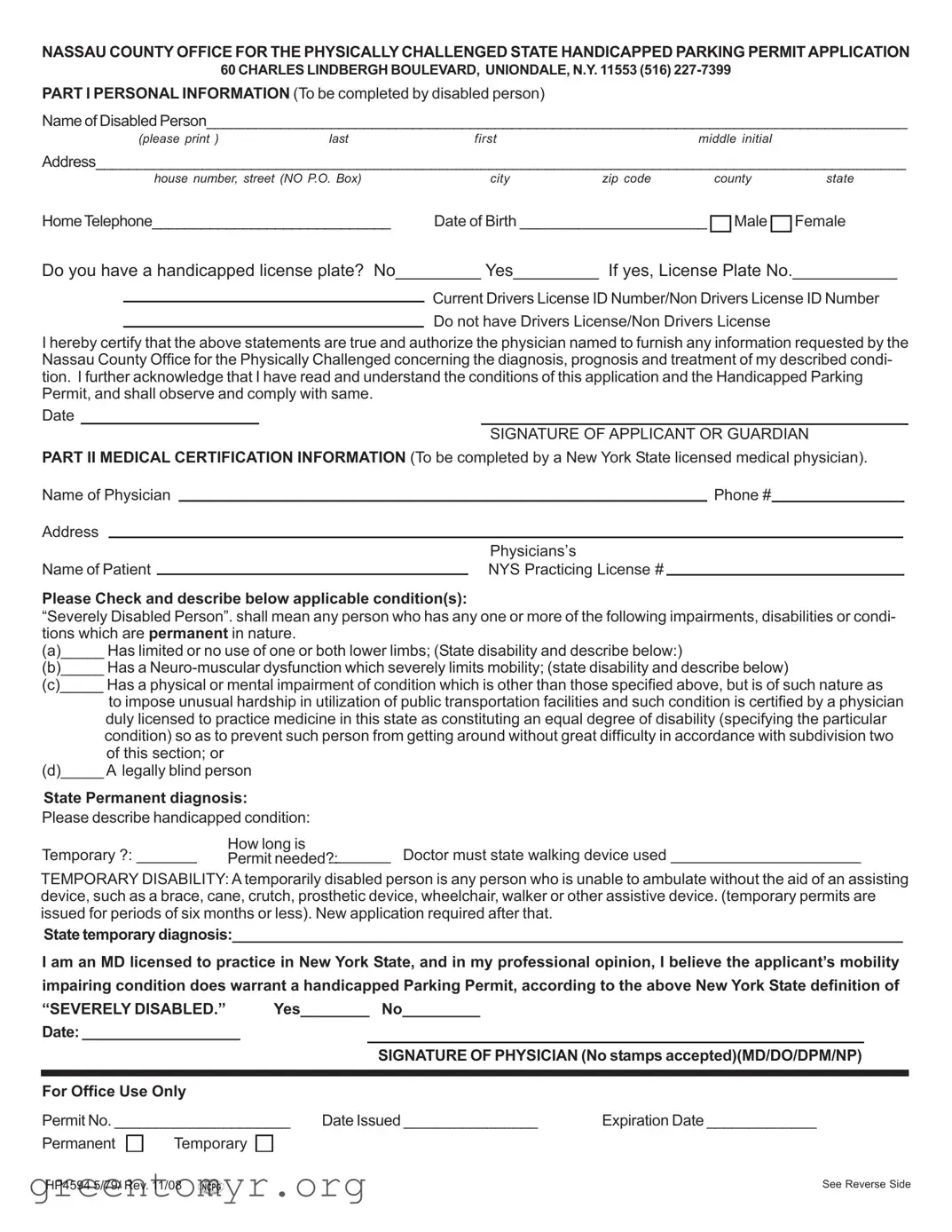
The Nassau Parking Application form is an essential document for residents of Nassau County seeking a handicapped parking permit. This application is designed specifically for individuals with severe disabilities that significantly impair their mobility. It consists of two main parts: personal information and medical certification. In the first section, applicants provide details such as their name, address, and contact information, along with their date of birth and gender. They must also indicate whether they possess a handicapped license plate. The second part requires a licensed New York State physician to certify the applicant's condition, detailing any physical impairments that justify the need for a permit. Important instructions accompany the form, emphasizing that it must be fully completed and signed, with no copies or faxes accepted. Additionally, it is crucial for applicants to include a self-addressed envelope for expedited processing. Understanding these key aspects is vital for ensuring a smooth application process and securing the necessary parking privileges.
| Fact Name | Description |
|---|---|
| Governing Authority | The application is governed by New York State laws regarding handicapped parking permits. |
| Eligibility | Applicants must be residents of Nassau County and have one or more severe disabilities that impair mobility. |
| Application Requirement | All applications must be fully completed and signed by the disabled person or their guardian. |
| Medical Certification | A licensed New York State medical physician must complete the medical certification section of the application. |
| Identification Requirement | Applicants must provide their New York State Drivers License Client ID number or a NYS ID card number. |
| Permit Issuance | Permits are issued in the name of the person with the disability, not necessarily the driver. |
| False Statements | Any false information provided by the applicant or physician may lead to denial of the permit. |
| Temporary Permits | Temporary permits are available for individuals unable to ambulate without an assisting device for six months or less. |
| Submission Guidelines | Applications must be original; copies or faxes will result in immediate denial. |
Filling out the Nassau Parking Application form is an important step for those seeking a handicapped parking permit. This process requires careful attention to detail to ensure that all necessary information is accurately provided. Once you have completed the form, you will submit it for review, and upon approval, you will receive your permit.
The Nassau Parking Application form is used to apply for a handicapped parking permit in Nassau County, New York. This permit allows individuals with severe disabilities that impair their mobility to park in designated handicapped spaces, making it easier for them to access public and private facilities.
To be eligible for a handicapped parking permit, you must be a resident of Nassau County and have one or more severe disabilities that significantly impair your ability to move around. The application must include a valid Nassau County street address; P.O. Boxes are not acceptable.
The application requires personal information about the disabled person, including their name, address, date of birth, and contact information. Additionally, it requires medical certification from a licensed New York State physician who must verify the applicant's mobility impairing condition. All sections of the application must be fully completed and signed.
No, the application must be completed in the name of the person with the disability. However, a guardian or caregiver can assist in filling out the form. It is crucial that all information pertains to the disabled applicant, not the person assisting them.
If the application is not fully completed or if any required information is missing, it will be denied. Additionally, any false statements made by the applicant or the physician will result in refusal to issue a permit. It is essential to review the application carefully before submission.
No, copies or faxes of the application will lead to immediate denial. Only original, signed applications will be processed. Ensure that the application is submitted in its original form.
To expedite the issuance of your permit, enclose a self-addressed envelope (size number 10) with your completed application. This will facilitate faster communication regarding your permit status once it has been approved.
Yes, temporary permits are issued for a maximum period of six months. If you require a permit beyond this duration, a new application must be submitted, along with updated medical certification. Ensure that your physician provides a clear statement regarding the temporary nature of your condition.
Filling out the Nassau Parking Application form can be straightforward, but many applicants make common mistakes that can delay the process or even lead to denial. One frequent error is failing to provide a complete address. The application specifically requires a Nassau County street address, and using a P.O. Box will result in immediate rejection. Ensure that every part of the address, including house number, street, city, and zip code, is accurately filled out.
Another mistake involves the medical certification section. Applicants often overlook the requirement for a licensed medical physician to complete this part. Only physicians with a valid New York State license can certify the applicant’s condition. Submitting a certification from a chiropractor or failing to include the physician’s signature will lead to automatic denial. It is crucial to verify that the physician's name, contact information, and license number are clearly stated.
Inaccuracies in personal information also pose a problem. Many individuals mistakenly provide incorrect or outdated information, such as an old phone number or an incorrect driver's license ID number. This can create confusion and hinder communication with the Nassau County Office for the Physically Challenged. Double-checking all personal details before submission is essential to avoid these pitfalls.
Some applicants forget to answer all questions on the form. Each section must be fully completed, and leaving any question unanswered can lead to delays. This includes the medical certification section, where specific conditions must be described in detail. Providing comprehensive information helps the reviewing office make informed decisions.
Moreover, applicants often neglect to include required documentation, such as a copy of the disabled applicant's ID. This is a crucial component that must accompany the application. Failing to include this documentation can result in immediate denial, so it’s wise to gather all necessary materials before submitting the application.
Lastly, many individuals do not read the instructions carefully. The form explicitly states that any false statements made by the applicant or the physician will lead to refusal of the permit. Understanding the requirements and adhering to them is vital for a successful application. By avoiding these common mistakes, applicants can streamline the process and increase their chances of receiving a handicapped parking permit.
When applying for a handicapped parking permit in Nassau County, several additional forms and documents may be required to support your application. These documents help ensure that all necessary information is accurately provided and that the application is processed efficiently. Below is a list of forms commonly used alongside the Nassau Parking Application form.
Gathering these documents in advance can help streamline the application process and reduce delays. Ensure that all information is accurate and complete to facilitate a smooth approval for your handicapped parking permit.
The Nassau Parking Application form is similar to several other documents that serve various purposes related to disability and parking permits. Here are eight documents that share similarities with the Nassau Parking Application form:
When filling out the Nassau Parking Application form, it is important to follow specific guidelines to ensure a smooth process. Below are four things you should and shouldn't do:
Understanding the Nassau Parking Application form can be challenging, and several misconceptions often arise. Here are eight common misunderstandings, along with clarifications to help navigate the application process.
This is not true. Any person with a qualifying disability can apply for a permit, regardless of whether they drive. Children and non-drivers are also eligible.
Only a licensed medical physician in New York State can complete this section. Chiropractors are not permitted to certify the application.
Submitting copies or faxes of the application will lead to immediate denial. The original, fully completed application is required.
Temporary disabilities also qualify for a permit. If a person is unable to ambulate without assistance for six months or less, they can apply for a temporary permit.
The application requires a physical street address in Nassau County. P.O. Boxes are not accepted.
The application must be signed by the disabled individual or their guardian. It cannot be signed by anyone else.
It is essential to include a copy of the disabled applicant's New York State Driver's License or ID card with the application.
Any false statement made by the applicant or the physician can lead to the refusal of the permit. Honesty is crucial when completing the application.
Filling out the Nassau Parking Application form correctly is essential to obtaining a handicapped parking permit. Here are some key takeaways to keep in mind:
By following these guidelines, you can help ensure a smoother application process for your handicapped parking permit.