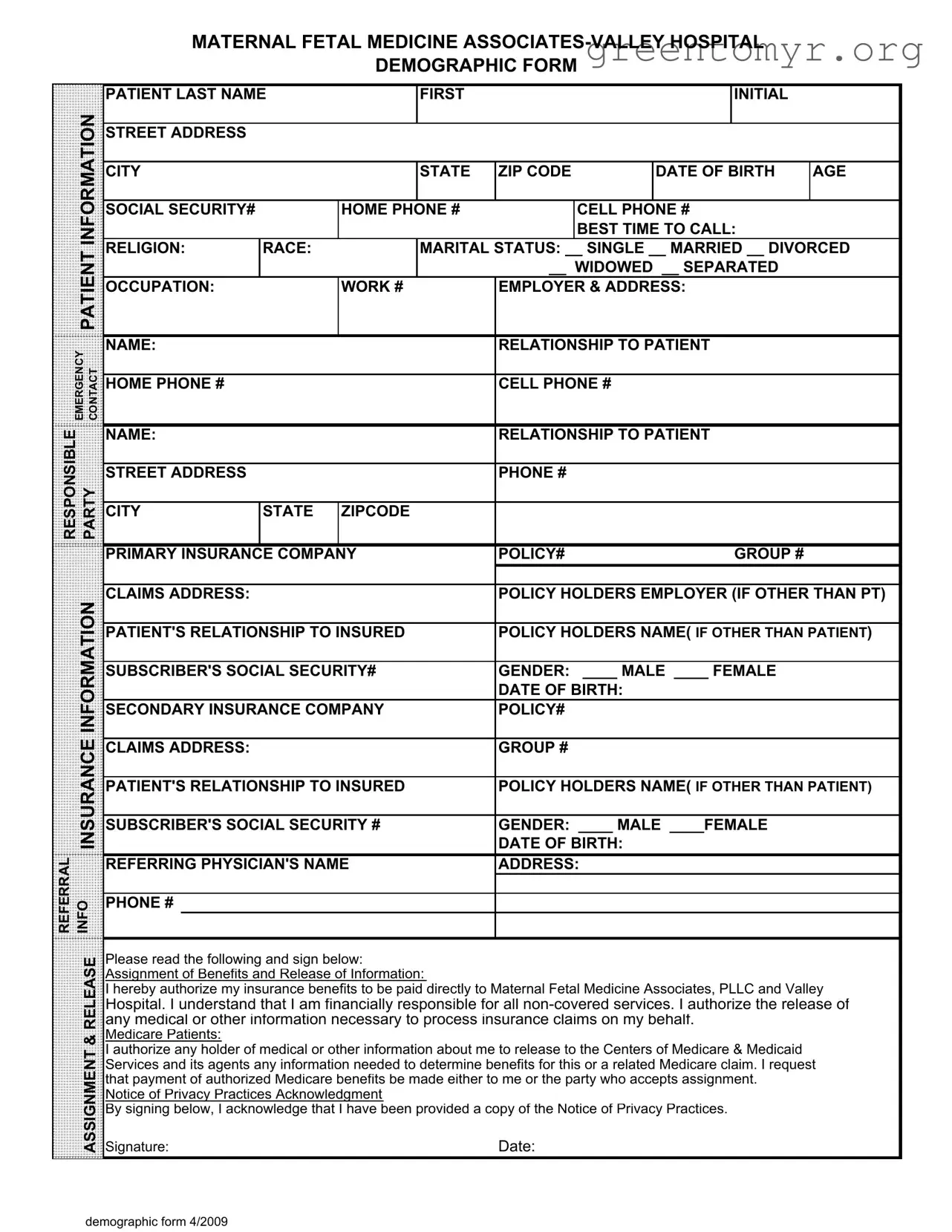
The Patient Demographics form is a crucial document that collects essential information about patients seeking care at Maternal Fetal Medicine Associates and Valley Hospital. This form gathers personal details such as the patient's name, address, and contact information, ensuring that healthcare providers can reach out when necessary. It also includes vital demographic data, including date of birth, age, gender, and marital status, which help in tailoring medical care to individual needs. The form requests information about the patient's insurance coverage, including primary and secondary insurance details, policy numbers, and the relationship of the insured to the patient. Emergency contact information is also captured, ensuring that a designated person can be reached in case of urgent situations. Additionally, the form contains a section for patients to authorize the release of medical information and assign benefits to the healthcare providers, streamlining the claims process with insurance companies. Understanding the significance of this form is essential for both patients and healthcare providers, as it lays the foundation for effective communication and care delivery.
MATERNAL FETAL MEDICINE
DEMOGRAPHIC FORM
PATIENT LAST NAME |
FIRST |
INITIAL |
|
INFORMATION |
|
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
|
STATE |
ZIP CODE |
DATE OF BIRTH |
AGE |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
SOCIAL SECURITY# |
|
HOME PHONE # |
|
CELL PHONE # |
|
|||
|
|
|
|
|
|
|
|
BEST TIME TO CALL: |
|
|
|
PATIENT |
RELIGION: |
RACE: |
|
MARITAL STATUS: __ SINGLE __ MARRIED __ DIVORCED |
|||||
|
|
|
|
|
|
__ WIDOWED __ SEPARATED |
|
|||
|
|
|
|
|
|
|
|
|||
|
|
OCCUPATION: |
|
WORK # |
EMPLOYER & ADDRESS: |
|
||||
|
|
|
|
|
|
|
|
|
|
|
EMERGENCY CONTACT |
NAME: |
|
|
|
RELATIONSHIP TO PATIENT |
|
||||
|
|
|
|
|
|
|
|
|
||
HOME PHONE # |
|
|
|
CELL PHONE # |
|
|
||||
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
||
RESPONSIBLE |
|
NAME: |
|
|
|
RELATIONSHIP TO PATIENT |
|
|||
PARTY |
|
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
PHONE # |
|
|
||||
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
STATE |
ZIPCODE |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
PRIMARY INSURANCE COMPANY |
POLICY# |
GROUP # |
|
|||||
|
|
|
|
|
|
|
|
|||
|
INFORMATION |
CLAIMS ADDRESS: |
|
|
|
POLICY HOLDERS EMPLOYER (IF OTHER THAN PT) |
||||
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT'S RELATIONSHIP TO INSURED |
POLICY HOLDERS NAME( IF OTHER THAN PATIENT) |
||||||||
|
|
|||||||||
|
|
|
|
|
|
|||||
|
|
SUBSCRIBER'S SOCIAL SECURITY# |
GENDER: ____ MALE ____ FEMALE |
|
||||||
|
|
|
|
|
|
|
DATE OF BIRTH: |
|
|
|
|
|
SECONDARY INSURANCE COMPANY |
POLICY# |
|
|
|||||
|
INSURANCE |
|
|
|
|
|
|
|
|
|
|
CLAIMS ADDRESS: |
|
|
|
DATE OF BIRTH: |
|
|
|||
|
|
|
|
|
GROUP # |
|
|
|||
|
|
PATIENT'S RELATIONSHIP TO INSURED |
POLICY HOLDERS NAME( IF OTHER THAN PATIENT) |
|||||||
|
|
|
|
|
|
|||||
|
|
SUBSCRIBER'S SOCIAL SECURITY # |
GENDER: ____ MALE ____FEMALE |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
REFERRAL |
INFO |
REFERRING PHYSICIAN'S NAME |
ADDRESS: |
|
|
|||||
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
PHONE # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RELEASE |
Please read the following and sign below: |
|
|
|
|
||||
|
Assignment of Benefits and Release of Information: |
|
|
|
|
|||||
|
|
|
|
|
|
|||||
|
|
I hereby authorize my insurance benefits to be paid directly to Maternal Fetal Medicine Associates, PLLC and Valley |
||||||||
|
|
Hospital. I understand that I am financially responsible for all |
||||||||
|
|
any medical or other information necessary to process insurance claims on my behalf. |
|
|||||||
|
& |
Medicare Patients: |
|
|
|
|
|
|
|
|
|
I authorize any holder of medical or other information about me to release to the Centers of Medicare & Medicaid |
|
||||||||
|
ASSIGNMENT |
|
||||||||
|
Signature: |
|
|
|
Date: |
|
|
|||
|
|
Services and its agents any information needed to determine benefits for this or a related Medicare claim. I request |
||||||||
|
|
that payment of authorized Medicare benefits be made either to me or the party who accepts assignment. |
|
|||||||
|
|
Notice of Privacy Practices Acknowledgment |
|
|
|
|
||||
|
|
By signing below, I acknowledge that I have been provided a copy of the Notice of Privacy Practices. |
|
|||||||
demographic form 4/2009
| Fact Name | Details |
|---|---|
| Purpose of the Form | The Patient Demographics form collects essential information about the patient for medical and billing purposes. |
| Required Information | It includes personal details such as name, address, date of birth, and insurance information. |
| Governing Laws | This form complies with HIPAA regulations to protect patient privacy and ensure confidentiality. |
| Emergency Contact | Patients must provide an emergency contact, including their relationship and phone numbers. |
Completing the Patient Demographics form is an essential step in ensuring that the healthcare provider has accurate and up-to-date information about the patient. This information will be used for scheduling appointments, billing, and communication regarding the patient's care. Follow these steps to fill out the form correctly.
The Patient Demographics form collects essential information about patients to ensure that healthcare providers have accurate and up-to-date records. This information helps in identifying patients, processing insurance claims, and facilitating effective communication. By providing details such as your name, address, date of birth, and insurance information, you enable the healthcare team to deliver personalized care and streamline administrative processes.
The form requires various details, including:
Providing complete and accurate information is crucial for your care and insurance processing.
Your privacy is a top priority. The healthcare provider is required to follow strict regulations regarding the confidentiality of your personal information. By signing the form, you acknowledge that you have received a copy of the Notice of Privacy Practices. This document outlines how your information will be used and protected. Additionally, only authorized personnel will have access to your data, ensuring it remains secure.
If you have any questions or need assistance while filling out the Patient Demographics form, do not hesitate to ask the staff for help. They are there to assist you. You can also review the form thoroughly before submitting it to ensure all information is correct. Clear communication is key, so feel free to express any concerns or seek clarification on any section of the form.
Completing the Patient Demographics form accurately is crucial for ensuring that healthcare providers can deliver the best possible care. However, individuals often make mistakes that can lead to complications in their medical treatment or billing processes. Here are seven common errors to avoid.
One frequent mistake is providing incomplete contact information. Patients sometimes forget to include their full street address or omit their cell phone number. This can create difficulties for healthcare providers trying to reach patients for appointments or important updates. Ensuring that all fields are filled out completely helps maintain clear communication.
Another common error involves inaccuracies in the social security number. A single digit entered incorrectly can lead to significant issues, especially when it comes to insurance claims. Patients should double-check this information to ensure it matches their official documents, as discrepancies can delay processing.
Many individuals also overlook the section regarding insurance information. Failing to provide the correct policy number or the name of the insurance company can result in denied claims. It is vital to have the insurance card on hand when filling out the form to ensure that all details are accurate.
Additionally, some patients neglect to specify their emergency contact information. This detail is essential in case of an emergency, as it allows healthcare providers to reach someone who can make decisions on the patient’s behalf. Including a reliable contact can make a significant difference in urgent situations.
Another mistake often made is not indicating the relationship to the responsible party. If a patient is not the one paying for the services, it is important to clarify this relationship to avoid confusion later on. This detail ensures that billing goes to the correct person and that all parties are informed about the patient’s care.
Patients sometimes forget to indicate their marital status, which can be relevant for insurance purposes and healthcare decisions. Providing this information helps healthcare providers understand the patient's support system and any potential legal considerations regarding medical decisions.
Lastly, individuals may fail to sign the release of information section. This signature is crucial for allowing healthcare providers to communicate with insurance companies and process claims efficiently. Without it, delays can occur, impacting both the patient’s care and billing processes.
By being aware of these common mistakes and taking the time to fill out the Patient Demographics form carefully, patients can help ensure a smoother healthcare experience. Accurate information not only facilitates effective communication but also supports timely and appropriate medical care.
The Patient Demographics form is a crucial document that collects essential information about a patient. However, it is often accompanied by several other forms and documents that serve various purposes within the healthcare system. Below is a list of commonly used documents that complement the Patient Demographics form.
These documents work together with the Patient Demographics form to create a comprehensive profile of the patient, ensuring that healthcare providers have the necessary information to deliver effective and efficient care.
When filling out the Patient Demographics form, it is important to follow specific guidelines to ensure accuracy and completeness. Here are seven things to do and not to do:
Understanding the Patient Demographics form is crucial for both patients and healthcare providers. Here are seven common misconceptions about this form:
By addressing these misconceptions, patients can approach the Patient Demographics form with clarity and confidence.
When completing the Patient Demographics form, it is essential to provide accurate and comprehensive information. Here are key takeaways to consider: