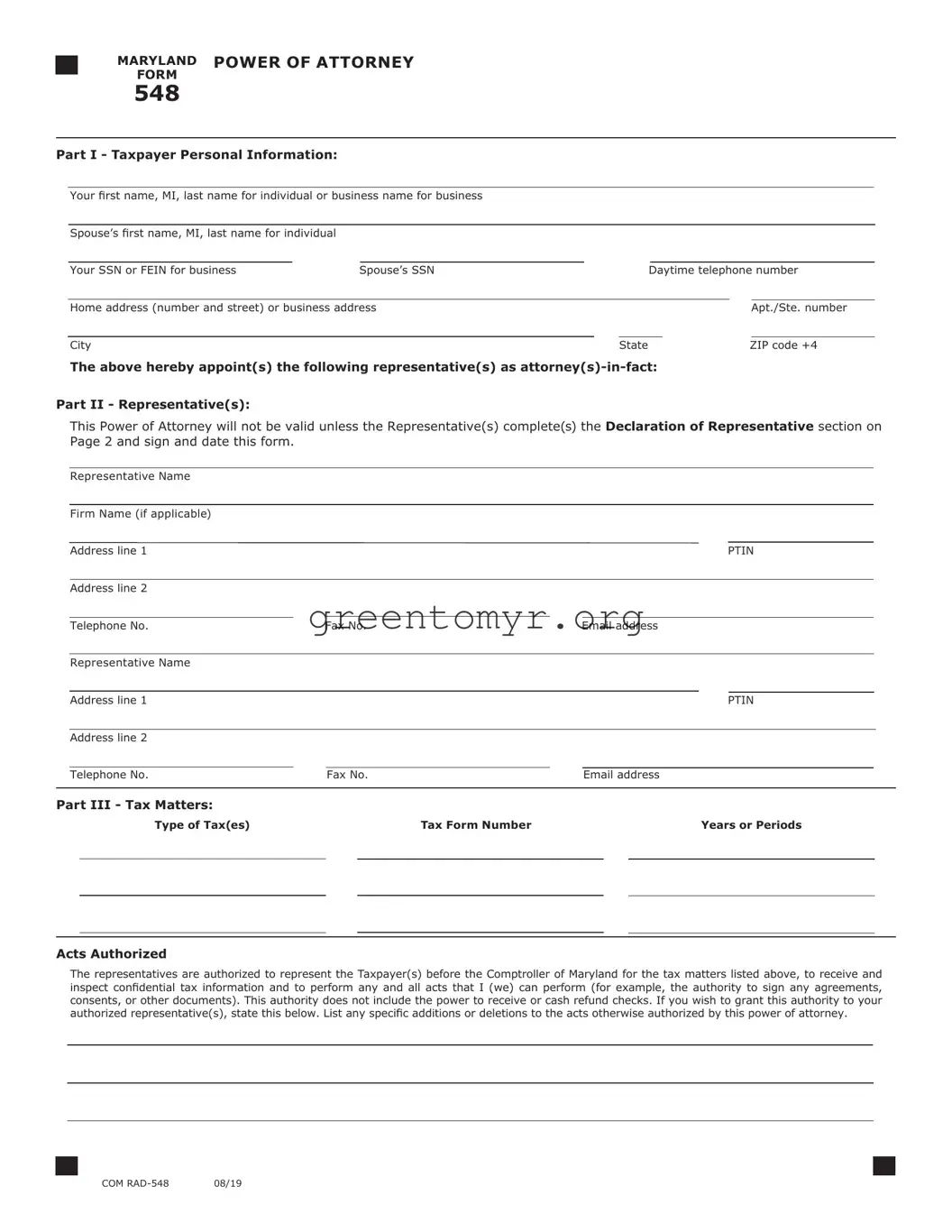
Understanding your tax situation can often feel overwhelming, especially when it comes to navigating the paperwork involved. One essential tool in managing your tax affairs effectively is the Tax Power of Attorney form, commonly known as Form 548. This form allows you to designate an individual to act on your behalf in dealings with the IRS, ensuring your interests are represented in important tax matters. By filing Form 548, you give someone you trust the authority to discuss your tax issues, receive confidential tax information, and make decisions on your behalf. Whether it’s addressing a tax audit, negotiating a payment plan, or simply obtaining advice on various tax matters, having a representative can provide peace of mind. Importantly, understanding the specific details about who can be appointed, the powers granted, and the process for revoking the authority when needed is crucial for anyone considering this option. With the right knowledge, you can take charge of your tax situation and ensure that you are adequately supported in your financial decisions.
■ |
|
MARYLAND |
POWER OF ATTORNEY |
|
|
|
|
|
|
|||||
|
FORM |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
548 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Part I - Taxpayer Personal Information: |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|||||||
|
Your first name, MI, last name for individual or business name for business |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
||||
|
Spouse’s first name, MI, last name for individual |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|||||||
|
Your SSN or FEIN for business |
Spouse’s SSN |
|
Daytime telephone number |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
||||
|
Home address (number and street) or business address |
|
|
|
|
Apt./Ste. number |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
|
State |
|
|
ZIP code +4 |
|
||
The above hereby appoint(s) the following representative(s) as
Part II - Representative(s):
This Power of Attorney will not be valid unless the Representative(s) complete(s) the Declaration of Representative section on Page 2 and sign and date this form.
Representative Name
|
Firm Name (if applicable) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address line 1 |
|
|
|
|
|
|
|
|
PTIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address line 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Telephone No. |
Fax No. |
Email address |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Representative Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address line 1 |
|
|
|
|
|
|
|
|
PTIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address line 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone No. |
|
Fax No. |
|
Email address |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
||
Part III - Tax Matters: |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Type of Tax(es) |
|
|
Tax Form Number |
|
|
|
|
Years or Periods |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Acts Authorized
The representatives are authorized to represent the Taxpayer(s) before the Comptroller of Maryland for the tax matters listed above, to receive and inspect confidential tax information and to perform any and all acts that I (we) can perform (for example, the authority to sign any agreements, consents, or other documents). This authority does not include the power to receive or cash refund checks. If you wish to grant this authority to your authorized representative(s), state this below. List any specific additions or deletions to the acts otherwise authorized by this power of attorney.
■ |
COM |
■ |
■ |
MARYLAND |
POWER OF ATTORNEY |
Page 2 |
FORM |
|
|
|
|
548 |
|
|
Taxpayer’s SSN or FEIN |
|
Taxpayer’s Name |
Retention/Revocation of Prior Power(s) of Attorney
By filing this power of attorney form, you automatically revoke all earlier power(s) of attorney on file with the Comptroller of Maryland for the same tax matters and years or periods covered by this document.
If you do not want to revoke a prior power of attorney, check here □

You must attach a copy of any Power of Attorney you want to remain in effect.
Signature of Taxpayer(s)
If a tax matter concerns a joint return, both spouses must sign if joint representation is requested. If signed by a corporate officer, partner, guardian, tax matters partner, executor, receiver, administrator, or trustee on behalf of the Taxpayer, I certify that I have the authority to execute this form on behalf of the Taxpayer. If other than the Taxpayer, print the name here and sign below.
Your signature |
Date |
|
|
Spouse’s signature if filing jointly |
Date |
Title, if business taxpayer or if other than individual taxpayer
Telephone number if other than the Taxpayer
If not signed and dated, this power of attorney will not be processed.
Declaration of Representative Representative(s) must complete this section and sign below.
Under penalties of perjury, I declare that
•I am not currently under suspension or disbarment from practice within the State of Maryland or in any jurisdiction;
•I have verified the identity of the taxpayer described under Taxpayer Personal Information and that the person signing as the authorized taxpayer is the same person described under Taxpayer Personal Information;
•I am aware of regulations governing the practice of attorneys, certified public accountants, public accountants, enrolled agents and others; and the penalties for false or fraudulent statements provided;
•I am authorized to represent in Maryland, the Taxpayer(s) identified for the tax matter(s) specified herein; and I am one of the following:
1.A member in good standing of the bar of the highest court of the jurisdiction shown below.
2.A Certified Public Accountant duly qualified to practice in the jurisdiction shown below.
3.An Enrolled Agent.
Attach
4.A Maryland Registered Individual Tax Preparer.
5.A bona fide officer of the Taxpayer.
6.A
7.A member of the Taxpayer’s immediate family (spouse, parent, child, grandparent, grandchild,
8.A general partner of the Taxpayer (partnership).
9.A fiduciary for the Taxpayer (Estate or trust).
10.Other (attach statement).
Jurisdiction (state)
Signature
Identification Number
(Bar, CPA, EA, Certification or Federal Employer Identification Number)
Date
An incomplete Form 548 will not be processed.
■ |
COM |
■ |
| Fact Name | Description |
|---|---|
| Form Title | Tax Power of Attorney (POA) Form 548 |
| Purpose | This form allows a taxpayer to designate an individual to represent them before the IRS. |
| IRS Availability | The form is available on the IRS website and can be downloaded for use. |
| Authorized Representations | The appointed representative can make decisions regarding tax matters on behalf of the taxpayer. |
| Required Signatures | Both the taxpayer and the representative must sign the form to validate it. |
| Governing Law | The form is governed by federal tax laws under the Internal Revenue Code. |
| Duration of Authority | The authority granted lasts until the taxpayer revokes it or the representative is replaced. |
| Limitations | Some decisions, like filing a fraudulent return, cannot be granted through this form. |
| Filing Requirements | A taxpayer should submit the form to the IRS along with any tax return or notice. |
| State-Specific Forms | Many states have their own versions of this form that comply with specific state laws. |
Filling out the Tax POA Form 548 is an important step if you require someone to represent you before the IRS. This process allows you to grant authority to a trusted individual, like an accountant or tax attorney, so they can act on your behalf. It involves various sections of the form where you’ll need to enter specific information about yourself, your representative, and the scope of authority you wish to grant.
The Tax Power of Attorney (POA) Form 548 is a document that allows a taxpayer to designate an individual, typically a tax professional or advisor, to act on their behalf regarding tax matters. This can include handling communications with tax authorities, filing returns, and accessing tax records. By granting this authority, taxpayers can ensure that their tax affairs are managed effectively, even if they are unable to do so themselves.
Taxpayers can appoint an individual of their choosing as their representative, as long as that person is qualified. This typically includes certified public accountants (CPAs), enrolled agents, attorneys, or other professionals who have a background in tax matters. It's important to ensure that the designated representative understands the taxpayer's needs and can competently handle tax-related issues.
To complete Form 548, follow these general steps:
Make sure to review the form for accuracy before submitting it to ensure all details are correct and the authority is clearly defined.
Yes, once completed, Form 548 should be submitted to the appropriate tax authority. Depending on your situation, this might include the IRS or state tax agencies. It is recommended to keep a copy for your records, as well as a confirmation of submission, to track the appointment of your representative.
Yes, a taxpayer can revoke the Power of Attorney at any time. This typically requires submitting a revocation notice to the same tax authority where the original Form 548 was sent. It is advisable to inform the representative as well, ensuring that they no longer act on your behalf and that your tax matters are handled as you desire.
If a taxpayer suspects that their representative is not acting in their best interest, they have the right to revoke the Power of Attorney immediately. Additionally, it may be necessary to assess potential misconduct. Taxpayers can consider contacting legal counsel or filing a complaint with relevant professional oversight organizations if warranted. It is essential to ensure that the appointed representative is trustworthy and aligned with your tax needs.
When individuals fill out the Tax Power of Attorney (POA) Form 548, several common mistakes can lead to delays or issues with their tax filings. Understanding these mistakes can help ensure that the form is submitted correctly, allowing for a smoother process.
One frequent error is failing to provide required personal information. Taxpayers must include their full name, address, and Social Security number or Employer Identification Number. Omitting any of this information can cause processing delays.
Another common mistake involves the selection of the representative. Some individuals may appoint someone who is not authorized to act as their representative. It’s crucial to ensure that the selected person meets the IRS requirements to avoid complications.
Additionally, the duration of the power of attorney can often be misinterpreted. Taxpayers must clearly specify whether the POA is for a specific time or until revoked. Not indicating this properly may lead to confusion about the authority granted.
The signature section is another area prone to mistakes. Many people forget to sign or date the form. Failure to provide a signature can result in rejection of the form, leading to additional paperwork and delays.
Completing the IRS Form 548 incorrectly also includes using outdated forms. Using an old or incorrect version of the POA can cause issues, so individuals must ensure they are using the latest form available on the IRS website.
Moreover, not checking the details of the form can lead to errors. Simple mistakes, such as misspellings in names or incorrect tax years, can cause problems. Always reviewing the information before submission can save time and hassle.
Finally, individuals often underestimate the value of providing additional documentation. In some cases, including copies of identification or other supporting documents might be necessary. Such items can verify identity and clarify the authority being granted.
By recognizing these common mistakes, individuals can better navigate the process of filling out Tax POA Form 548. Ensuring accuracy and completeness will lead to a more efficient handling of tax matters.
When completing a Tax Power of Attorney (POA) form 548, several other forms and documents may also be required or beneficial to have on hand. These documents can help streamline the tax filing process or provide additional information needed for specific situations. Below is a list of common forms used in conjunction with the Tax POA.
Being aware of these forms and their purposes can help ease the tax preparation process. Collecting the necessary documents ensures all aspects of your tax situation are addressed accurately and efficiently.
When filling out Form 548 for Tax Power of Attorney (POA), it is essential to approach the task carefully. Here are crucial do's and don'ts to keep in mind:
Taking these actions seriously can help ensure that your submission is processed efficiently and without issues.
This form is useful for individuals as well as businesses. Anyone needing to authorize a representative for tax matters should consider using it.
Submitting the form does not ensure any specific outcome. Approval or acceptance is subject to IRS review and policies.
You only need to file the form if you wish to change your representative or if you want to authorize a different individual.
A Power of Attorney can be revoked at any time, as long as the appropriate procedures are followed.
The Tax POA Form 548 is generally straightforward. Most individuals can fill it out without needing legal help.
While attorneys can serve as representatives, you may also designate other qualified individuals. This can include family members or trusted friends.
The form is specifically for federal tax matters, but it does not replace any state-specific authorizations that may be needed.
While it allows a representative to access your tax information, the form does not give them access to any unauthorized data.
It is essential to keep a copy for your records. This helps ensure both you and your representative are aligned on the authority granted.
Designating a representative does not eliminate your responsibility. You remain accountable for any tax matters and decisions.
When dealing with the IRS and needing to authorize someone else to act on your behalf, the Tax POA form 548 plays an important role. Here are some crucial points to consider when filling out and using this form:
Following these takeaways can help ensure that the process goes smoothly and that your representative can effectively assist you with your tax matters.