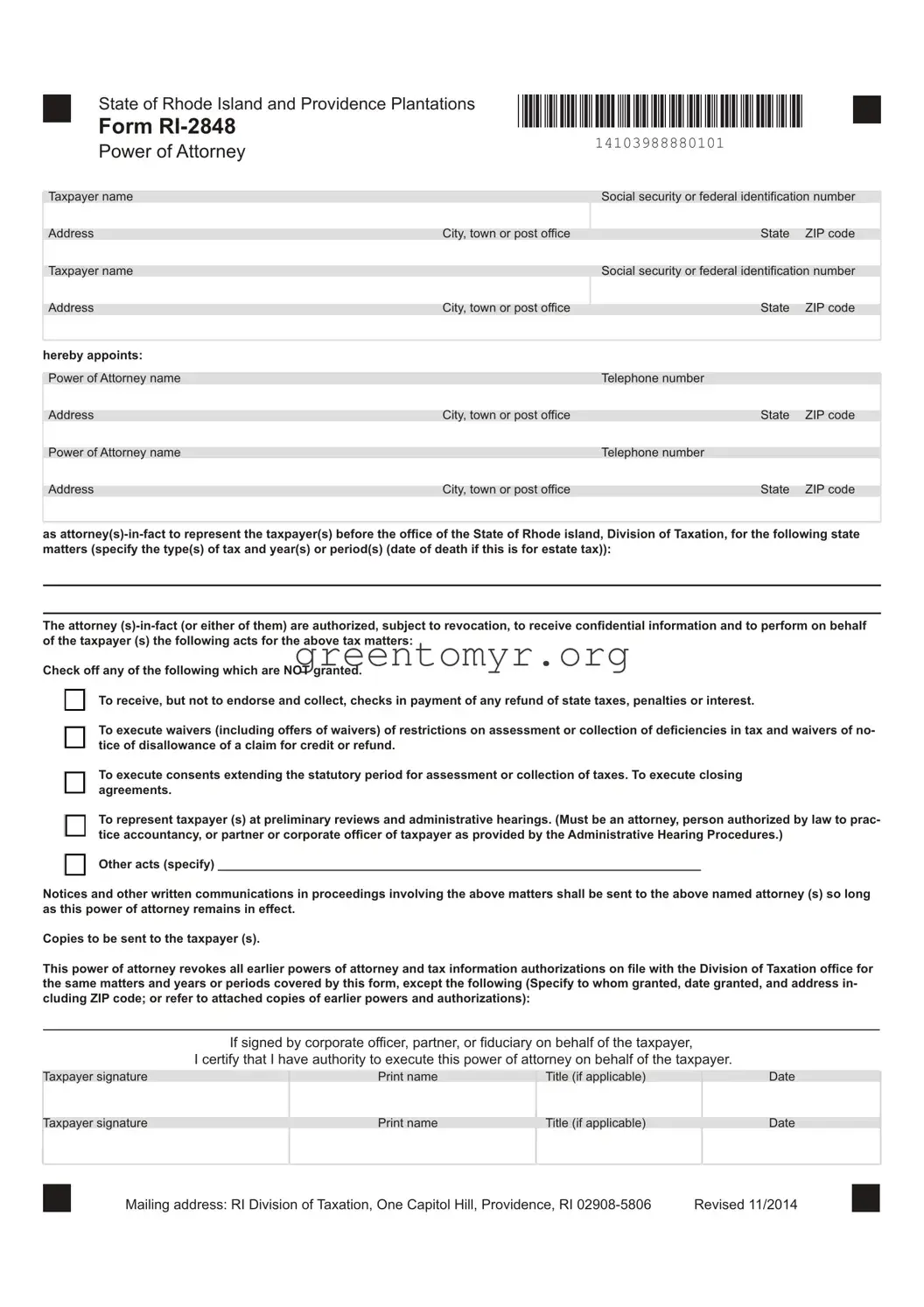
The Tax Power of Attorney (POA) form RI-2848 is an important document for anyone who needs to appoint someone else to handle their tax matters. This form allows an individual to designate an authorized representative, such as an accountant or attorney, to communicate with the Rhode Island Division of Taxation on their behalf. By using the RI-2848, taxpayers can ensure their interests are represented accurately without needing to be present for every discussion or decision-making instance. The form requires you to provide essential details about both the taxpayer and the representative, including names, addresses, and Social Security numbers. It also outlines the specific powers granted to the representative, which can range from receiving confidential information to signing tax returns. The flexibility of this form helps simplify tax situations, whether you’re dealing with individual taxes, business filings, or audits. Completing the RI-2848 properly not only streamlines communication with tax authorities but also provides peace of mind knowing that your tax matters are in capable hands.
■ |
State of Rhode Island and Providence Plantations |
Illllll lllll lllll lllll lllll lllll lllll lllll lllll lllll lllll lllll 111111111111111111 |
■ |
Form |
|||
|
Power of Attorney |
14103988880101 |
|
Taxpayer name |
|
Social security or federal identification number |
|
|
|
|
|
|
|
Address |
City, town or post office |
State |
ZIP code |
|
|
|
|
|
|
Taxpayer name |
|
Social security or federal identification number |
|
|
|
|
|
|
|
Address |
City, town or post office |
State |
ZIP code |
|
|
|
|
|
|
hereby appoints: |
|
|
|
|
|
|
|
|
|
Power of Attorney name |
|
Telephone number |
|
|
|
|
|
|
|
Address |
City, town or post office |
State |
ZIP code |
|
|
|
|
|
|
Power of Attorney name |
|
Telephone number |
|
|
|
|
|
|
|
Address |
City, town or post office |
State |
ZIP code |
|
as
The attorney
Check off any of the following which are NOT granted.
[ I
[ I
□

□

□

To receive, but not to endorse and collect, checks in payment of any refund of state taxes, penalties or interest.
To execute waivers (including offers of waivers) of restrictions on assessment or collection of deficiencies in tax and waivers of no- tice of disallowance of a claim for credit or refund.
To execute consents extending the statutory period for assessment or collection of taxes. To execute closing agreements.
To represent taxpayer (s) at preliminary reviews and administrative hearings. (Must be an attorney, person authorized by law to prac- tice accountancy, or partner or corporate officer of taxpayer as provided by the Administrative Hearing Procedures.)
Other acts (specify) ______________________________________________________________________
Notices and other written communications in proceedings involving the above matters shall be sent to the above named attorney (s) so long as this power of attorney remains in effect.
Copies to be sent to the taxpayer (s).
This power of attorney revokes all earlier powers of attorney and tax information authorizations on file with the Division of Taxation office for the same matters and years or periods covered by this form, except the following (Specify to whom granted, date granted, and address in- cluding ZIP code; or refer to attached copies of earlier powers and authorizations):
If signed by corporate officer, partner, or fiduciary on behalf of the taxpayer,
I certify that I have authority to execute this power of attorney on behalf of the taxpayer.
Taxpayer signature |
Print name |
Title (if applicable) |
Date |
|
|
|
|
|
|
Taxpayer signature |
Print name |
Title (if applicable) |
Date |
|
|
|
|
|
■ |
Mailing address: RI Division of Taxation, One Capitol Hill, Providence, RI |
Revised 11/2014 |
■ |
■ |
State of Rhode Island and Providence Plantations |
Illllll lllll lllll lllll lllll lllll lllll lllll lllll lllll lllll lllll 111111111111111111 |
■ |
Form |
|||
|
Power of Attorney |
14103988880102 |
|
This declaration must be completed by the attorney, certified public accountant, licensed public accountant, or enrolled agent. I declare that I am not currently under suspension or disbarment from practice before the Division of Taxation and that:
□

□

□

[ I
I am a member in good standing of the bar of the highest court of the jurisdiction indicated below; or
I am duly qualified to practice as a certified public accountant in the jurisdiction indicated below; or
I am a licensed public accountant in the jurisdiction indicated below.
I am actively enrolled to practice before the Internal Revenue Service.
Designation |
Jurisdiction |
Signature |
Date |
(Attorney, CPA, LPA or enrolled agent) |
(State, etc) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If the power of attorney is granted to a person other than an attorney, certified public accountant, or licensed public accountant, or enrolled agent, it must be witnessed or notarized below.
The person (s) signing as or for the taxpayer (s): (Check and complete ONE.)
|
|
□ |
|
|
|
is/are known to and signed in the presence of the two disinterested witnesses whose signatures appear here: |
|
|
|
|
|
||||
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of witness |
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of witness |
Date |
|
|
|
|
||||
|
LJ |
|
appeared this day before a notary public and acknowledged this power of attorney as a voluntary act and deed |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of notary |
Date |
NOTARIAL SEAL
■■
| Fact Name | Description |
|---|---|
| Purpose | The RI-2848 form is used to authorize an individual to represent you in tax matters before the Rhode Island Division of Taxation. |
| Eligibility | Any individual or entity can complete the form to designate a representative, such as an attorney, accountant, or enrolled agent. |
| Filing Requirements | This form must be submitted when you want someone else to handle your tax affairs on your behalf. It does not eliminate your responsibility for your tax obligations. |
| State Law | The RI-2848 is governed by the Rhode Island General Laws, specifically under Title 44 relating to taxation. |
| Signatures | The taxpayer must sign and date the form before submission. The representative must also provide their information, including a signature. |
| Submission | The completed RI-2848 can be submitted via mail or electronically, depending on the preferences of the Rhode Island Division of Taxation. |
Preparing to fill out the RI-2848 form is an essential step in obtaining the necessary power of attorney for tax purposes. After completing this form, you will be able to designate someone to act on your behalf in matters related to your state taxes. Follow these steps carefully to ensure that you fill out the form accurately.
After you submit the completed RI-2848 form, your designated representative should be able to engage with the tax authorities on your behalf. It’s advisable to confirm with your representative that they have received the necessary approval to act in your interests.
The Tax POA Form RI-2848, also known as Power of Attorney, is a document that allows you to authorize someone to act on your behalf regarding tax matters in Rhode Island. This person, often referred to as your agent, can communicate with the Rhode Island Division of Taxation, file returns, and make decisions related to your tax obligations. It's important to select an agent you trust because they will have the authority to discuss your tax situation with tax authorities.
To properly fill out the RI-2848 form, follow these steps:
Make sure to double-check all information for accuracy before submitting the form to avoid any complications.
After completing the RI-2848 form, send it to the Rhode Island Division of Taxation. You can either mail it directly to their office or submit it in person, depending on your preference. Consider keeping a copy of the signed form for your records. If you experience difficulties or have questions, contacting the Division of Taxation can provide further guidance on the submission process.
The RI-2848 form does not have a fixed expiration date but can be revoked at any time. If you wish to terminate the authority granted to your agent, you must notify the Rhode Island Division of Taxation in writing. It's advisable to periodically review the powers you've granted, especially if your financial situation or trust with your agent changes. Keeping everything current helps ensure that your tax matters are handled efficiently.
When filling out the Tax POA (Power of Attorney) form RI-2848, people often make several common mistakes that can lead to delays or complications with the IRS. One frequent error is forgetting to include all required signatures. Without a valid signature from both the taxpayer and the representative, the form is incomplete. Ensure that both parties sign the form in the designated areas to avoid this problem.
Another mistake occurs when individuals fail to specify the exact tax matters for which the Power of Attorney is granted. The RI-2848 form asks for specific details regarding the tax issues being addressed. Leaving this section blank or providing vague descriptions can result in the IRS rejecting the authorization. Clearly outline the tax matters to ensure that your representative has the authority to act on your behalf.
Many also overlook the importance of updating the information on the form. If there have been changes to your representative’s information, such as address or phone number, it’s essential to reflect these updates on the form. Failing to provide current information can lead to communication issues between the IRS, the taxpayer, and the representative, creating unnecessary complications.
Lastly, individuals may neglect to keep a copy of the completed Tax POA form for their records. After submitting the RI-2848 form, it’s wise to maintain a copy in case any questions arise later. Having a copy can help clarify any misunderstandings down the line and ensure that you and your representative are on the same page about the authorization.
The Tax Power of Attorney (POA) form RI-2848 is essential for anyone seeking to authorize an individual to represent them in matters concerning tax issues. In addition to this form, there are several other documents that can be useful in managing tax-related matters. Below is a list of these forms, each with a brief description to help you understand their purposes.
Having these forms at your disposal can facilitate smoother communication and ensure that all aspects of your tax affairs are managed effectively. Understanding the role of each document will empower you to make informed decisions regarding your tax representation and filings.
When completing the Tax Power of Attorney (POA) Form RI-2848, it’s essential to be careful and thorough. This form allows someone to represent you before the IRS, so accuracy is key. Below are ten important tips, presented as dos and don'ts, to ensure that your application is completed correctly.
By adhering to these guidelines, you can ensure a smoother experience while handling your Tax POA form. Accuracy and attention to detail will benefit you and your appointed representative in navigating tax matters efficiently.
The Tax Power of Attorney (POA) form RI-2848 is often misunderstood. Here are seven common misconceptions:
Understanding these misconceptions can lead to better management of your tax affairs. Always review the requirements thoroughly and consult with trusted individuals if needed.
When dealing with the Tax POA form RI-2848, it’s essential to understand its purpose and how to fill it out correctly. Here are some key takeaways to help you navigate this process:
Completing the RI-2848 form correctly can enhance communication with tax authorities and streamline any tax-related matters you may have.