When dealing with tax matters, having a trusted representative by your side can make the process smoother and less stressful. The Tax Power of Attorney (POA) IL-2848 form is an essential tool for taxpayers in Illinois who want to authorize someone, such as a family member, accountant, or attorney, to handle their tax affairs on their behalf. This form grants the designated individual the authority to communicate directly with the Illinois Department of Revenue (IDOR) and manage issues related to individual income taxes, sales taxes, and more. Filling out the IL-2848 correctly ensures that your chosen representative can access necessary tax information, receive notifications, and make valid decisions regarding your tax matters. Key details about the taxpayer and the representative must be disclosed on the form, and it must be submitted to ensure that the permission is granted. Understanding the nuances of the IL-2848 can empower you to choose the right representative and simplify your interactions with tax authorities.
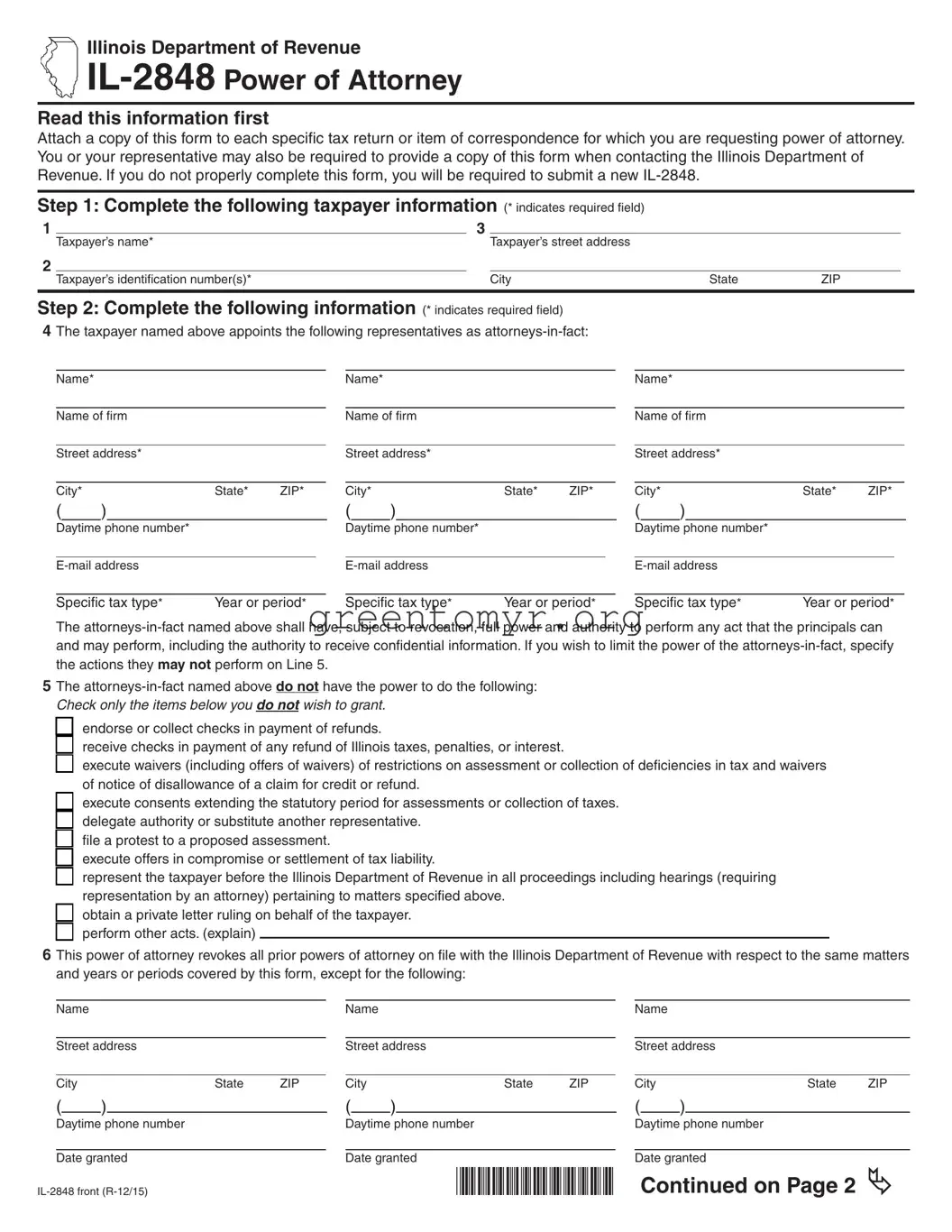
Illinois Department of Revenue
Read this information frst
Attach a copy of this form to each specifc tax return or item of correspondence for which you are requesting power of attorney. You or your representative may also be required to provide a copy of this form when contacting the Illinois Department of Revenue. If you do not properly complete this form, you will be required to submit a new
Step 1: Complete the following taxpayer information (* indicates required feld)
1 |
|
3 |
|
|
|
|
|
Taxpayer’s name* |
|
Taxpayer’s street address |
|
|
|
2 |
|
|
|
|
|
|
|
Taxpayer’s identifcation number(s)* |
|
City |
State |
ZIP |
|
|
|
|
|
|
|
|
Step 2: Complete the following information (* indicates required feld)
4 The taxpayer named above appoints the following representatives as
Name* |
|
|
|
|
|
|
|
Name* |
|
|
|
|
|
|
|
Name* |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Name of frm |
|
|
|
|
Name of frm |
|
|
|
|
Name of frm |
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Street address* |
|
|
|
|
Street address* |
|
|
|
|
Street address* |
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
City* |
|
|
|
State* |
ZIP* |
City* |
|
|
|
State* |
ZIP* |
City* |
|
|
|
State* |
ZIP* |
||||||||
( |
|
) |
|
|
|
|
( |
|
) |
|
|
|
|
( |
|
) |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Daytime phone number* |
|
|
|
|
Daytime phone number* |
|
|
|
|
Daytime phone number* |
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Specifc tax type* |
Year or period* |
|
Specifc tax type* |
Year or period* |
|
Specifc tax type* |
Year or period* |
||||||||||||||||||
The
5 The
□
 endorse or collect checks in payment of refunds.
endorse or collect checks in payment of refunds.
□ receive checks in payment of any refund of Illinois taxes, penalties, or interest.
□ execute waivers (including offers of waivers) of restrictions on assessment or collection of defciencies in tax and waivers of notice of disallowance of a claim for credit or refund.
□
 execute consents extending the statutory period for assessments or collection of taxes. □
execute consents extending the statutory period for assessments or collection of taxes. □
 delegate authority or substitute another representative.
delegate authority or substitute another representative.
□
 fle a protest to a proposed assessment.
fle a protest to a proposed assessment.
□
 execute offers in compromise or settlement of tax liability.
execute offers in compromise or settlement of tax liability.
□
 represent the taxpayer before the Illinois Department of Revenue in all proceedings including hearings (requiring representation by an attorney) pertaining to matters specifed above.
represent the taxpayer before the Illinois Department of Revenue in all proceedings including hearings (requiring representation by an attorney) pertaining to matters specifed above.
□
 obtain a private letter ruling on behalf of the taxpayer. □
obtain a private letter ruling on behalf of the taxpayer. □
 perform other acts. (explain)
perform other acts. (explain)
6 This power of attorney revokes all prior powers of attorney on fle with the Illinois Department of Revenue with respect to the same matters and years or periods covered by this form, except for the following:
Name |
|
|
|
|
|
Name |
|
|
|
|
|
Name |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||||||||
Street address |
|
|
|
Street address |
|
|
|
Street address |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
City |
|
|
State |
ZIP |
|
City |
|
|
State |
ZIP |
|
City |
|
State |
ZIP |
|||
( |
|
) |
|
|
|
( |
|
) |
|
|
|
( |
|
) |
|
|
||
|
Daytime phone number |
Daytime phone number |
Daytime phone number |
||
|
|
|
|
|
|
|
Date granted |
Date granted |
Date granted |
||
*565201110* |
|
Continued on Page 2 |
|||
7 Copies of notices and other written communications addressed to the taxpayer in proceedings involving the matters listed on the front of this form should be sent to the following:
Name |
|
|
|
|
|
Name |
|
|
|
|
|
Name |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||||||||
Street address |
|
|
|
Street address |
|
|
|
Street address |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
City |
|
|
State |
ZIP |
|
City |
|
|
State |
ZIP |
|
City |
|
State |
ZIP |
|||
( |
|
) |
|
|
|
( |
|
) |
|
|
|
( |
|
) |
|
|
||
Daytime phone number |
|
|
|
Daytime phone number |
|
|
|
Daytime phone number |
|
|||||||||
Step 3: Complete the following if the power of attorney is granted to an attorney, a certifed public accountant, or an enrolled agent
I declare that I am not currently under suspension or disbarment and that I am
•a member in good standing of the bar of the highest court of the jurisdiction indicated below; or
•duly qualifed to practice as a certifed public accountant in the jurisdiction indicated below; or
•enrolled as an agent pursuant to the requirements of United States Treasury Department Circular Number 230.
Check one: □Attorney |
□C.P.A. □Enrolled agent |
|
|
|
Jurisdiction (state(s), etc.) |
Signature |
Date |
||
Check one: □Attorney |
□C.P.A. □Enrolled agent |
|
|
|
Jurisdiction (state(s), etc.) |
Signature |
Date |
||
Check one: □Attorney |
□C.P.A. □Enrolled agent |
|
|
|
Jurisdiction (state(s), etc.) |
Signature |
Date |
Step 4: Taxpayer’s signature
If signing as a corporate offcer, partner, fduciary, or individual on behalf of the taxpayer, I certify that I have the authority to execute this power of attorney on behalf of the taxpayer.
Taxpayer’s signature |
Print name |
Title, if applicable |
Date |
|
|
|
|
Spouse’s signature |
Print name |
Title, if applicable |
Date |
|
|
|
|
If corporation or partnership, signature of offcer or partner |
Print name |
Title, if applicable |
Date |
Complete the following if the power of attorney is granted to a person other than an attorney, a certifed public accountant, or an enrolled agent
If the power of attorney is granted to a person other than an attorney, a certifed public accountant, or an enrolled agent, this document must be witnessed or notarized below. Please check and complete one of the following:
Any person signing as or for the taxpayer |
|
|
|
|
□ |
is known to and this document is signed in the presence of |
|
||
|
the two disinterested witnesses whose signatures appear here. |
|
||
|
|
|
|
|
|
Signature of witness |
Date |
|
|
|
|
|
|
|
|
Signature of witness |
Date |
|
|
□ |
appeared this day before a notary public and acknowledged |
|
||
|
this power of attorney as his or her voluntary act and deed. |
|
||
|
|
|
|
Notary seal |
|
Signature of notary |
Date |
||
This form is authorized as outlined under the Illinois Income Tax Act. Disclosure of this information is required. Failure to provide information could result in a penalty.
*565202110*
| Fact Name | Description |
|---|---|
| Purpose | The IL-2848 form is used to grant a Power of Attorney for tax matters in the state of Illinois. |
| Governing Law | This form is governed by Illinois Department of Revenue regulations. |
| Authorized Representatives | Taxpayers can designate one or more representatives to handle their tax affairs. |
| Duration | The authorization remains in effect until it is revoked or the final tax issues are resolved. |
| Eligibility | Both individuals and businesses can use this form to appoint a representative. |
| Submission Method | The completed IL-2848 form can be submitted electronically or by mail to the Illinois Department of Revenue. |
| Revocation | Taxpayers can revoke the Power of Attorney by submitting a written notice any time before the resolution of tax matters. |
Filling out the Tax POA IL-2848 form is a straightforward process, and completing it accurately is essential for effective tax representation. Follow the steps below to ensure that the form is filled out correctly.
After submitting the form, the designated representative will be able to interact with the tax authority on your behalf regarding the specified matters. Keep a copy of the completed form for your records, as it may be important for future reference.
The Tax POA IL-2848 form is a Power of Attorney authorization used in the state of Illinois. It allows a designated individual, known as an attorney-in-fact, to represent a taxpayer before the Illinois Department of Revenue. This form enables the appointed person to handle tax matters on behalf of the taxpayer, including filing returns, negotiating tax liabilities, and receiving confidential information.
Taxpayers can appoint anyone they trust as their attorney-in-fact. This could include:
It’s important to choose someone who understands tax laws and can effectively manage the taxpayer's affairs.
To complete the IL-2848 form, follow these steps:
Ensure all fields are filled out accurately to avoid delays in processing.
The completed IL-2848 form should be submitted to the Illinois Department of Revenue. It can typically be sent via mail, fax, or electronically, depending on the department’s current submission policies. Always check for the latest guidelines from the Illinois Department of Revenue for the best submission method.
Processing times may vary based on the volume of requests received by the Illinois Department of Revenue. Generally, it may take a few weeks for the form to be processed. If the submission is incomplete or incorrect, it may take longer. It's advisable to follow up with the department if you haven't received confirmation within a reasonable timeframe.
When filling out the Tax Power of Attorney (POA) IL-2848 form, people often make several common mistakes that can delay processing or lead to complications. A careful review of the form before submission can help avoid these pitfalls.
One frequent error is omitting the required personal information. It is crucial to include the taxpayer's full name, address, and Social Security number (or Employer Identification Number) accurately. Missing or incorrect information creates confusion and can result in the form being rejected.
Another common mistake is failing to properly complete the representative section. Many people overlook the need to provide the representative's contact information or to specify the types of tax matters the representative is authorized to handle. Without this clarity, the IRS might not validate the representative's authority.
Many taxpayers also neglect to check all boxes that apply to their specific needs. The form has different sections for different tax categories, such as income tax, estate tax, and more. If the correct boxes are not marked, the Tax POA may not cover the necessary issues.
Inaccurate signatures or dates often cause headaches too. The form must be signed by the taxpayer, and if the signature is not valid or the date is missing, the IRS could reject the application. It's important to double-check that all required signatures are included.
People sometimes forget to specify the exact tax years for which the representative is authorized to act. This oversight can limit the power granted to the representative and could prevent them from accessing the taxpayer's full financial history as needed.
Another mistake involves misunderstanding the representative's relationship with the taxpayer. Sometimes individuals assume that any family member can serve as a representative without understanding the rules governing such relationships. Knowing who can serve as a representative is vital to ensure compliance.
Alongside all these errors, it is imperative to pay attention to deadlines. Submitting the form late can have significant repercussions. Various IRS timelines dictate when a Power of Attorney needs to be filed, and missing these deadlines can hinder the representation process.
Finally, some taxpayers fail to keep a copy of the completed form. Retaining a copy is essential for reference and can be invaluable if questions arise later. Keeping organized records ensures smoother communication between the taxpayer, the representative, and the IRS.
The Tax Power of Attorney (POA) IL-2848 form allows individuals to authorize someone to represent them before the Illinois Department of Revenue. This document is often accompanied by several other forms to ensure that the representation is comprehensive and effective. The following are four other forms and documents commonly used alongside the IL-2848.
Using these forms effectively helps mitigate misunderstandings and fosters clearer communication between the taxpayer and the appointed representative. Proper documentation ensures compliance and supports a smoother tax process.
The IRS Form IL-2848, also known as the Power of Attorney, serves specific purposes in tax-related situations. Several other documents share similarities with this form in terms of granting authorization or designating representation. Below are eight documents comparable to the IL-2848:
Filling out the Tax POA IL-2848 form accurately is important. Here are some dos and don'ts to consider:
Understanding the Tax POA IL-2848 form is essential for anyone involved in tax matters. Here are nine common misconceptions about this form, along with clarifications:
Understanding the Tax POA IL-2848 form is crucial for anyone needing representation in tax matters. Here are some key takeaways to help you navigate its requirements effectively:
Taking the time to understand these key points will streamline your experience with tax representation. Review the requirements carefully, and ensure that each section of the form is filled out completely and accurately to avoid delays.